
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
CORONA Main Coronavirus thread
- Thread starter Heliobas Disciple
- Start date
-
- Tags
- coronavirus
Tom McDowell
BAMN
14% of Recovered Covid-19 Patients in Guangdong Tested Positive Again
By Li Liuqian, Huang Shulun and Han Wei

Guangdong health authority found 14% of recovered coronavirus patients tested positive again in later check-ups. Photo: Bloomberg
About 14% of patients who recovered from the novel coronavirus and were discharged from hospitals in southern China’s Guangdong province were tested positive again in later check-ups, according to the local health authority. A positive test suggests the recovered patients may still carry the virus, adding complexity to efforts to control the outbreak.
There is no clear conclusion on why it happens and whether such patients could still be infectious, said Song Tie, deputy director of the Guangdong Center of Disease Control And Prevention (Guangdong CDC), at a Tuesday briefing.
According to the preliminary assessment, experts believed the patients are still recovering from lung infections and have yet to be fully healthy, according to Song.
According to the latest treatment guidelines for the Covid-19 issued by the National Health Commission, patients can be considered recovered and released from hospital when their throat or nose swabs show up negative in two consecutive tests, with a CT scan indicating no lung lesions, and when they have no obvious symptoms such as fever.
The guidelines suggest recovered patients should monitor their health and limit outdoor activities for two weeks after leaving the hospital, and check in for retesting in following weeks.
Some patients’ test results returned to positive in the follow-up checks, said Li Yueping, director of the intensive care unit at Guangzhou No.8 People's Hospital at the briefing.
Read more
Caixin’s coverage of the new coronavirus
The No.8 People's Hospital has found 13 discharged patients that tested positive again, although none showed renewed symptoms, according to Li. Nucleic acid tests for 104 close contacts of the patients all found negative results, said Li.
Cai Weiping, director of the Infectious Diseases Division of the No.8 People's Hospital, told Caixin that the positive results in the recovered patients were all found from anal swabs, a method rarely used in other parts of the country. Their results were in the “weak positive” range, said Cai.
The national treatment guideline only requires tests from throat or nose swabs for suspected patients as the virus is believed to spread mainly via respiratory droplets produced when an infected person coughs or sneezes. But research by Guangzhou Medical University found the virus in fecal samples, suggesting a new path of transmission. Some hospitals in Guangdong have since adopted the anal swab in virus tests.
Cai said it is still unclear whether the virus detected in the recovered patients is still active. There is also the possibility of a discrepancy in samples, he said.
Song at Guangdong CDC said the province is preparing to put those recovered patients who re-tested positive under concentrated observation. Health authorities will also step up monitoring of discharged patients and their condition as they recover, said Song.
By the end of Monday, Guangdong reported 1,347 infections and 805 recoveries. The death toll reached seven, official data showed.
Similar cases of recovered patients testing positive have been reported elsewhere in China.
Last week, a patient initially discharged after recovering in southwestern Sichuan province’s Chengdu city was readmitted after testing positive again in later check-ups.
Health authorities in the southern island province of Hainan also confirmed that some recovered patients had tested positive again. The authorities required discharged patients to stay home under quarantine for 14 days, and allowed them to be released after both throat and anal swab tests showed negative.
Contact reporter Han Wei (weihan@caixin.com)
====
.
By Li Liuqian, Huang Shulun and Han Wei
Guangdong health authority found 14% of recovered coronavirus patients tested positive again in later check-ups. Photo: Bloomberg
About 14% of patients who recovered from the novel coronavirus and were discharged from hospitals in southern China’s Guangdong province were tested positive again in later check-ups, according to the local health authority. A positive test suggests the recovered patients may still carry the virus, adding complexity to efforts to control the outbreak.
There is no clear conclusion on why it happens and whether such patients could still be infectious, said Song Tie, deputy director of the Guangdong Center of Disease Control And Prevention (Guangdong CDC), at a Tuesday briefing.
According to the preliminary assessment, experts believed the patients are still recovering from lung infections and have yet to be fully healthy, according to Song.
According to the latest treatment guidelines for the Covid-19 issued by the National Health Commission, patients can be considered recovered and released from hospital when their throat or nose swabs show up negative in two consecutive tests, with a CT scan indicating no lung lesions, and when they have no obvious symptoms such as fever.
The guidelines suggest recovered patients should monitor their health and limit outdoor activities for two weeks after leaving the hospital, and check in for retesting in following weeks.
Some patients’ test results returned to positive in the follow-up checks, said Li Yueping, director of the intensive care unit at Guangzhou No.8 People's Hospital at the briefing.
Read more
Caixin’s coverage of the new coronavirus
The No.8 People's Hospital has found 13 discharged patients that tested positive again, although none showed renewed symptoms, according to Li. Nucleic acid tests for 104 close contacts of the patients all found negative results, said Li.
Cai Weiping, director of the Infectious Diseases Division of the No.8 People's Hospital, told Caixin that the positive results in the recovered patients were all found from anal swabs, a method rarely used in other parts of the country. Their results were in the “weak positive” range, said Cai.
The national treatment guideline only requires tests from throat or nose swabs for suspected patients as the virus is believed to spread mainly via respiratory droplets produced when an infected person coughs or sneezes. But research by Guangzhou Medical University found the virus in fecal samples, suggesting a new path of transmission. Some hospitals in Guangdong have since adopted the anal swab in virus tests.
Cai said it is still unclear whether the virus detected in the recovered patients is still active. There is also the possibility of a discrepancy in samples, he said.
Song at Guangdong CDC said the province is preparing to put those recovered patients who re-tested positive under concentrated observation. Health authorities will also step up monitoring of discharged patients and their condition as they recover, said Song.
By the end of Monday, Guangdong reported 1,347 infections and 805 recoveries. The death toll reached seven, official data showed.
Similar cases of recovered patients testing positive have been reported elsewhere in China.
Last week, a patient initially discharged after recovering in southwestern Sichuan province’s Chengdu city was readmitted after testing positive again in later check-ups.
Health authorities in the southern island province of Hainan also confirmed that some recovered patients had tested positive again. The authorities required discharged patients to stay home under quarantine for 14 days, and allowed them to be released after both throat and anal swab tests showed negative.
Contact reporter Han Wei (weihan@caixin.com)
14% of Recovered Covid-19 Patients in Guangdong Tested Positive Again - Caixin Global
14% of Recovered Covid-19 Patients in Guangdong Tested Positive Again - Unclear whether recovered patients who test positive remain infectious; none showed renewed symptoms, and none of their contacts tested positive for the virus
www.caixinglobal.com
.
jward
passin' thru
IIRC we have literally just a handful- like six or seven left : (I came across this film on infantile paralysis (polio) from 1949. It seems like that came in waves as well. So glad this doesn't hit children.
Wonder if there are any of those iron lungs left? It seems they moved equipment from community to community as it hit.
View: https://www.youtube.com/watch?v=bws4KI2u6tk
10 min
Epidemic's Children - 1940s Polio Epidemic Fundraising Film with Iron Lungs 84610 HD
But yes, immense gratitude that we'll not have to watch babies dying en masse...even hearts of stone have their limits.
 ((
((marsh
On TB every waking moment
I froze some milk in their plastic containers (Just unscrew top and use some of it as it expands when frozen.)CM......I ordered 3 10# cans of Morning Moo powdered milk to have for my grandsons.
Tom McDowell
BAMN
6 min ago
US could see a similar death rate to China if the virus spreads, says top infectious diseases doctor
From CNN's Ben Tinker
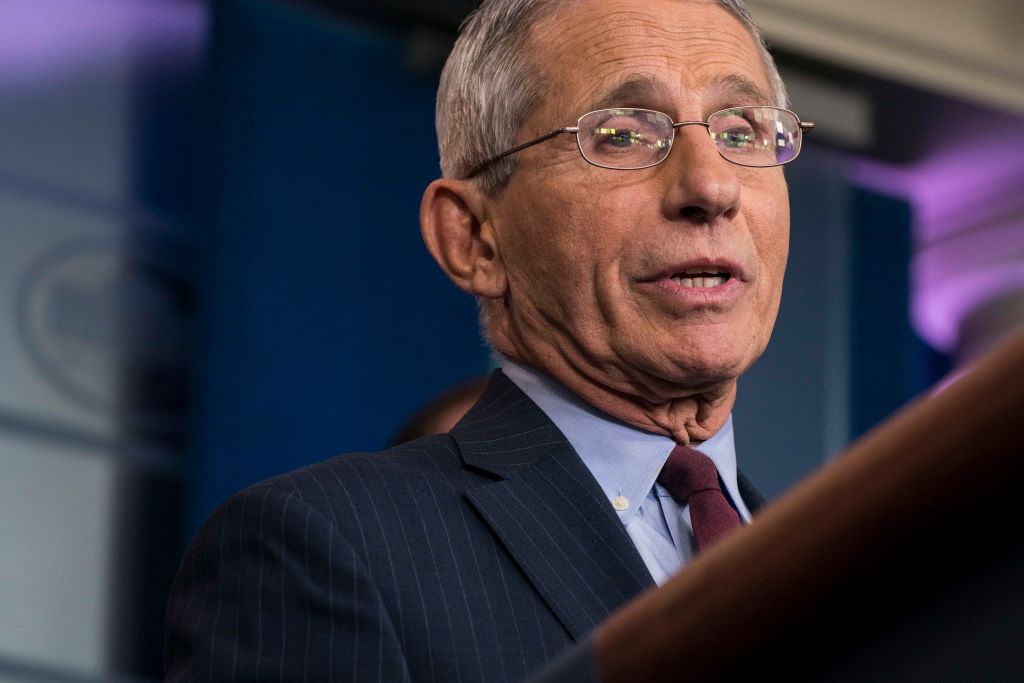
Anthony Fauci in the White House Briefing Room on January 31 in Washington, DC. Sarah Silbiger/Getty Images
Dr. Anthony Fauci, director of the US National Institute of Allergy and Infectious Diseases, told CNN the US needed more resources to fight the coronavirus outbreak, which has infected 53 people in the US.
“We’ve had a pandemic preparedness plan that we really developed in preparation for pandemic influenza, that we can extrapolate to this. We certainly need more resources, and that’s what you heard today with the supplemental request. Because we can only go a certain way with the resources we have,” Fauci said.
Death rate: Fauci added that the fatality rate of the outbreak could reach the same levels in the US as in China because there is no vaccine or cure available.
"I mean, the people who are dying who require intensive care, for example in an intensive care unit -- maybe even intubation for respiratory assistance in breathing -- the Chinese have that. They have a pretty good system, and yet you’re still seeing the 2% mortality. So it isn’t a question of, ‘they don’t have as good care as we have.’ So if, in fact, we do get a pandemic that does impact us in this country, I think you’re going to see comparable types of morbidity and mortality," he said.

 www.cnn.com
www.cnn.com
===
.
US could see a similar death rate to China if the virus spreads, says top infectious diseases doctor
From CNN's Ben Tinker
Anthony Fauci in the White House Briefing Room on January 31 in Washington, DC. Sarah Silbiger/Getty Images
Dr. Anthony Fauci, director of the US National Institute of Allergy and Infectious Diseases, told CNN the US needed more resources to fight the coronavirus outbreak, which has infected 53 people in the US.
“We’ve had a pandemic preparedness plan that we really developed in preparation for pandemic influenza, that we can extrapolate to this. We certainly need more resources, and that’s what you heard today with the supplemental request. Because we can only go a certain way with the resources we have,” Fauci said.
Death rate: Fauci added that the fatality rate of the outbreak could reach the same levels in the US as in China because there is no vaccine or cure available.
"I mean, the people who are dying who require intensive care, for example in an intensive care unit -- maybe even intubation for respiratory assistance in breathing -- the Chinese have that. They have a pretty good system, and yet you’re still seeing the 2% mortality. So it isn’t a question of, ‘they don’t have as good care as we have.’ So if, in fact, we do get a pandemic that does impact us in this country, I think you’re going to see comparable types of morbidity and mortality," he said.
February 26, 2020 coronavirus news
Europe's biggest coronavirus outbreak is in Italy, where more than 320 have been infected, while Iran has reported more than 90 cases and 15 deaths. Follow here for live updates.
===
.
marsh
On TB every waking moment
13:33min
Dr. John Campbell
COVID-19 Tuesday Morning
•Feb 25, 2020
marsh
On TB every waking moment
11:54 min
MEDCRAM Epidemic Update 25: Vaccine Developments, Italy's Response, and Mortality Rate Trends Dr. Roger Seheult
•Feb 25, 2020
L.A.B.
Goodness before greatness.
Containment-mitigation measures are AI-driven.
AI is not human. Remember that.
Be human and humane and American. I'm not saying hand all your stuff out to strangers. Just hold your head up and don't be afraid. Shit happens.
They blindfold horses to lead them out of a fire. Be calm and thoughtful or AI may blindfold you. No shit.
Very strange Helen. I’m not sure where your ideas about AI shaping responses comes from, but I have been (((thinking))) along those same lines for the last two days.
Almost get the sense HUMINT is taking orders from alphaindia.
I concur, help people where you can. There was no overt chaos yesterday when I was standing in a coffee shop and the person in front of me, a tatted up hardcore ex-banger type born again Christian asked the barista if they had elderberry tea...? (((Coincidence)))
I asked him ‘what was he looking for’ as he asked again elderberry tea.
Didn’t I just post yesterday about finding organic elderberry tea at the grocery store. I had 4-boxes in the car. I ended up giving one away. Handshakes and God bless You’s were exchanged.
I’ve spent the last three weeks getting people up to speed with self help info. From my neighbor a dentist to eager to learn co-workers. I don’t do bleeding heart stuff, I help those looking to help themselves and others.
Tom McDowell
BAMN
The Coronavirus Pandemic Is A Crisis Now Obvious To All
71,770 views
RT 36:00

Peak Prosperity
PROTECT yourself & your family by READING Chris' latest free report "Why Covid-19 Demands Our Full Attention" here: https://www.peakprosperity.com/why-co... Then WATCH UPDATE #30 HERE: https://youtu.be/fLYnomkC1fA
As 19th century German philosopher Arthur Schopenhauer claimed, “All truth passes through three stages: First, it is ridiculed. Second, it is violently opposed. Third, it is accepted as self-evident.”
After weeks of denial, and attacks on voices like Peak Prosperity who dared question the "Everything is fine!" narrative, world governments and their mass media partners are finally admitting that the coronavirus threat is real and serious.
The pandemic continues to spread across the globe, interestingly, largely in the northern hemisphere at this time. This may suggest it could migrate south as fall/winter arrives there, possibly returning northwards when the seasons change again.
Time will tell. Meanwhile, the markets continue their sell-off as the economic damage from the impairment of Asian supply chains become more apparent. How much further can they fall? A LOT if the virus continues to rage on for months.
As this crisis is now becoming more obvious to all, remember that your best time to prepare is BEFORE the panicked herd stampedes. Take the time you have now to keep plugging away at your preparations, so that you're secure and positioned to help should covid-19 hit your community.
===
.
If they were just monitored or "under observation", but not tested, they could have been asymptomatic but positive much earlier, within the "normal" period.Feb 25, 2020 08:50 PM
SOCIETY & CULTURE
Guangzhou Family Cluster Appears to Experience Extra-Long Covid-19 Incubation
By Huang Shulun and Dave Yin

Shared bikes block the entrance of a street in Guangzhou’s Liwan district. Photo: Liang Yingfei/Caixin
A family in South China’s Guangdong province may have experienced a Covid-19 incubation period of a month, another case that could challenge the widely held notion that the maximum period is around 14 days and raise questions about measures taken to prevent the spread of the virus.
Authorities in Guangzhou’s Liwan district announced (link in Chinese) over the weekend that several members of the family of six tested positive for Covid-19 following a near month-long quarantine after traveling to the city from the epicenter of the epidemic.
The Pan family took a train from Wuhan, Hubei province, to Guangzhou on Jan. 22, and were then placed under quarantine. On Feb. 20, one of them, identified as the “son-in-law,” developed a fever. He tested positive for the disease on Feb. 21, and his wife and a child were diagnosed the following day.
According to the local authorities, the family was under medical observation between Jan. 24 and Feb. 7, something routinely done in the district for those arriving from Hubei. Nothing unusual was reported during this period, and the monitoring was lifted.
If confirmed by scientists, the case would add to evidence that challenges the current medical understanding of the disease’s incubation period, or the time it takes for a growing pathogen to reach a quantity necessary to produce symptoms in the host.
A study of more than 1,099 coronavirus patients by Chinese scientists, published in early February as a preprint, or a paper that has not been peer reviewed, has already made the case that the incubation period could be as long as 24 days, rather than the 14-day maximum previously believed.
Meanwhile, Xinyang, a city in Central China’s Henan province, announced on Feb. 16 that local authorities had diagnosed a “highly unusual” case where a patient tested positive on a third screening, some 34 days after leaving Wuhan. Furthermore, a person in Zhongshan, Guangdong, who had undergone a routine two-week quarantine after arriving from Hubei on Jan. 26 tested positive almost a month later.
At a Feb. 18 press conference, Chinese epidemiologist Zhong Nanshan, who discovered the SARS coronavirus in 2003 and co-authored the 1,099-person study, said that he did not find the longer incubation periods to be strange, explaining that there are always exceptions.
Of the Covid-19 patients studied, 13 had incubation periods longer than 14 days, though the majority developed signs of illness within two to seven days of contracting the virus, Zhong said.
According to an article by German researchers in the New England Journal of Medicine, asymptomatic Covid-19 carriers may be contagious, and the widespread practice of screening based on symptoms may not be effective.
Many countries continue to use two-week quarantine periods as yardsticks for assessing citizens with potential infections.
On Feb. 24, Guangdong lowered its Covid-19 epidemic emergency response from level one, the country’s highest, to level two.
Contact reporter Dave Yin (davidyin@caixin.com) and editor Joshua Dummer (joshuadummer@caixin.com)
===Guangzhou Family Cluster Appears to Experience Extra-Long Covid-19 Incubation - Caixin Global
Guangzhou Family Cluster Appears to Experience Extra-Long Covid-19 Incubation - Case adds to evidence that symptoms may not emerge for longer than 14 days, raising questions about containment methodswww.caixinglobal.com
.

marsh
On TB every waking moment
Coronavirus Disease 2019 (COVID-19)
Coronavirus disease 2019 (COVID-19) is a virus (more specifically, a coronavirus) identified as the cause of an outbreak of respiratory illness first detected in Wuhan, China.
Updated CDC situation Report
Updated February 25, 2020
Background
CDC is responding to an outbreak of respiratory disease caused by a novel (new) coronavirus that was first detected in Wuhan City, Hubei Province, China and which has now been detected in 37 locations internationally, including cases in the United States. The virus has been named “SARS-CoV-2” and the disease it causes has been named “coronavirus disease 2019” (abbreviated “COVID-19”).
On January 30, 2020, the International Health Regulations Emergency Committee of the World Health Organization declared the outbreak a “public health emergency of international concernexternal icon” (PHEIC). On January 31, 2020, Health and Human Services Secretary Alex M. Azar II declared a public health emergency (PHE) for the United States to aid the nation’s healthcare community in responding to COVID-19.
Source and Spread of the Virus
Coronaviruses are a large family of viruses that are common in many different species of animals, including camels, cattle, cats, and bats. Rarely, animal coronaviruses can infect people and then spread between people such as with MERS-CoV, SARS-CoV, and now with this new virus (named SARS-CoV-2).
The SARS-CoV-2 virus is a betacoronavirus, like MERS-CoV and SARS-CoV. All three of these viruses have their origins in bats. The sequences from U.S. patients are similar to the one that China initially posted, suggesting a likely single, recent emergence of this virus from an animal reservoir.
Early on, many of the patients in the COVID-19 outbreak in Wuhan, China had some link to a large seafood and live animal market, suggesting animal-to-person spread. Later, a growing number of patients reportedly did not have exposure to animal markets, indicating person-to-person spread. Person-to-person spread has been reported outside China, including in the United States and other locations. Chinese officials report that sustained person-to-person spread in the community is occurring in China. In addition, other destinations have apparent community spread, meaning some people have been infected who are not sure how or where they became infected. Learn what is known about the spread of newly emerged coronaviruses.
Confirmed COVID-19 Cases Global Map

View larger image and see a list of locations
map icon
COVID-19 cases in the U.S.
Situation in U.S.
Imported cases of COVID-19 in travelers have been detected in the U.S. Person-to-person spread of COVID-19 also has been seen among close contacts of returned travelers from Wuhan, but at this time, this virus is NOT currently spreading in the community in the United States.
Illness Severity
Both MERS-CoV and SARS-CoV have been known to cause severe illness in people. The complete clinical picture with regard to COVID-19 is not fully understood. Reported illnesses have ranged from mild to severe, including illness resulting in death. Learn more about the symptoms associated with COVID-19.
There are ongoing investigations to learn more. This is a rapidly evolving situation and information will be updated as it becomes available.
Risk Assessment
Outbreaks of novel virus infections among people are always of public health concern. The risk from these outbreaks depends on characteristics of the virus, including how well it spreads between people, the severity of resulting illness, and the medical or other measures available to control the impact of the virus (for example, vaccine or treatment medications). The fact that this disease has caused illness, including illness resulting in death, and sustained person-to-person spread is concerning. These factors meet two of the criteria of a pandemic. As community spread is detected in more and more countries, the world moves closer toward meeting the third criteria, worldwide spread of the new virus.
The potential public health threat posed by COVID-19 is high, both globally and to the United States.
But individual risk is dependent on exposure.
- For the general American public, who are unlikely to be exposed to this virus at this time, the immediate health risk from COVID-19 is considered low.
- Under current circumstances, certain people will have an increased risk of infection, for example healthcare workers caring for patients with COVID-19 and other close contacts of persons with COVID-19. CDC has developed guidance to help in the risk assessment and management of people with potential exposures to COVID-19.
What May Happen
More cases are likely to be identified in the coming days, including more cases in the United States. It’s also likely that person-to-person spread will continue to occur, including in the United States. Widespread transmission of COVID-19 in the United States would translate into large numbers of people needing medical care at the same time. Schools, childcare centers, workplaces, and other places for mass gatherings may experience more absenteeism. Public health and healthcare systems may become overloaded, with elevated rates of hospitalizations and deaths. Other critical infrastructure, such as law enforcement, emergency medical services, and transportation industry may also be affected. Health care providers and hospitals may be overwhelmed. At this time, there is no vaccine to protect against COVID-19 and no medications approved to treat it. Nonpharmaceutical interventions would be the most important response strategy.
CDC Response
Global efforts at this time are focused concurrently on containing spread of this virus and mitigating the impact of this virus. The federal government is working closely with state, local, tribal, and territorial partners, as well as public health partners, to respond to this public health threat. The public health response is multi-layered, with the goal of detecting and minimizing introductions of this virus in the United States so as to reduce the spread and the impact of this virus. CDC is operationalizing all of its pandemic preparedness and response plans, working on multiple fronts to meet these goals, including specific measures to prepare communities to respond local transmission of the virus that causes COVID-19. There is an abundance of pandemic guidance developed in anticipation of an influenza pandemic that is being repurposed and adapted for a COVID-19 pandemic.
Highlights of CDC’s Response
- CDC established a COVID-19 Incident Management System on January 7, 2020. On January 21, CDC activated its Emergency Operations Center to better provide ongoing support to the COVID-19 response.
- The U.S. government has taken unprecedented steps with respect to travelin response to the growing public health threat posed by this new coronavirus:
- Effective February 2, at 5pm, the U.S. government suspended entry of foreign nationals who have been in China within the past 14 days.
- U.S. citizens, residents, and their immediate family members who have been in Hubei province and other parts of mainland China are allowed to enter the United States, but they are subject to health monitoring and possible quarantine for up to 14 days.
- CDC has issued the following travel guidance related to COVID-19:
- China — Level 3, Avoid Nonessential Travel — updated February 22;
- South Korea — Level 3, Avoid Nonessential Travel — updated February 24;
- Japan — Level 2, Practice Enhanced Precautions — updated February 22;
- Iran — Level 2, Practice Enhanced Precautions — issued February 23;
- Italy — Level 2, Practice Enhanced Precautions — issued February 23;
- Hong Kong — Level 1, Practice Usual Precautions — issued February 19.
- CDC also recommends that all travelers reconsider cruise ship voyages into or within Asia at this time.
- CDC is issuing clinical guidance, including:
- An interim Health Alert Network (HAN) Update to inform state and local health departments and healthcare professionals about this outbreak on February 1.
- On January 30, CDC published guidance for healthcare professionals on the clinical care of COVID-19 patients.
- On February 3, CDC posted guidance for assessing the potential risk for various exposures to COVID-19 and managing those people appropriately.
- CDC has deployed multidisciplinary teams to support state health departments with clinical management, contact tracing, and communications.
. CDC is shipping the test kits to laboratories CDC has designated as qualified, including U.S. state and local public health laboratories, Department of Defense (DOD) laboratories and select international laboratories. The test kits are bolstering global laboratory capacity for detecting SARS-CoV-2.")
This is a picture of CDC’s laboratory test kit for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). CDC is shipping the test kits to laboratories CDC has designated as qualified, including U.S. state and local public health laboratories, Department of Defense (DOD) laboratories and select international laboratories. The test kits are bolstering global laboratory capacity for detecting SARS-CoV-2.
resize iconView Larger
- CDC laboratories have supported the COVID-19 response, including:
- CDC has developed a real time Reverse Transcription-Polymerase Chain Reaction (rRT-PCR) test that can diagnose COVID-19 in respiratory samples from clinical specimens. On January 24, CDC publicly posted the assay protocol for this test.
- CDC has been uploading the entire genome of the viruses from reported cases in the United States to GenBank as sequencing was completed.
- CDC has grown the COVID-19 virus in cell culture, which is necessary for further studies, including for additional genetic characterization. The cell-grown virus was sent to NIH’s BEI Resources Repositoryexternal icon for use by the broad scientific community.
- While the immediate risk of this new virus to the American public is believed to be low at this time, everyone can do their part to help us respond to this emerging public health threat:
- It’s currently flu and respiratory disease season and CDC recommends getting a flu vaccine, taking everyday preventive actions to help stop the spread of germs, and taking flu antivirals if prescribed.
- If you are a healthcare provider, be on the look-out for people who recently traveled from China and have fever and respiratory symptoms.
- If you are a healthcare provider caring for a COVID-19 patient or a public health responder, please take care of yourself and follow recommended infection control procedures.
- If you have been in China or have been exposed to someone sick with COVID-19 in the last 14 days, you will face some limitations on your movement and activity. Please follow instructions during this time. Your cooperation is integral to the ongoing public health response to try to slow spread of this virus. If you develop COVID-19 symptoms, contact your healthcare provider, and tell them about your symptoms and your travel or exposure to a COVID-19 patient.
- For people who are ill with COVID-19, please follow CDC guidance on how to reduce the risk of spreading your illness to others.
We might want to be prepared for things to move even much faster, once kick-off begun...Then we would see the three days until anarchy theory kick in. Three days of food in most cities, less in most homes. Game on.
I think the "three days food theory" could be short circuited, where it's greatly shortened quick
as even a small % grasps that all the food will be gone in three days, they won't wait till then,
they'll overrun all the grocery stores that same day that that reality has dawned on them. Then,
everybody else seeing that happening, they'll also pile on, too. Stores could empty in day/night.
Panic Early, Beat the Rush!
- Shane
marsh
On TB every waking moment
Coronavirus Disease 2019 (COVID-19)
CDC provides credible COVID-19 health information to the U.S.
 www.cdc.gov
www.cdc.gov
More Releases from the CDC
- MMWR: Public Health Response to the Coronavirus Disease 2019 Outbreak— United StatesTUESDAY, FEBRUARY 25, 2020
- Interim Guidance for Public Health Personnel Evaluating Persons Under Investigation (PUIs) and Asymptomatic Close Contacts of Confirmed Cases at Their Home or Non-Home Residential SettingsMONDAY, FEBRUARY 24, 2020
- Coronavirus Disease 2019 Information for Travel (New Travel Alerts)MONDAY, FEBRUARY 24, 2020
- CDC in Action: Preparing Communities for Potential Spread of COVID-19SUNDAY, FEBRUARY 23, 2020
- Frequently Asked Questions and Answers: Coronavirus Disease-2019 (COVID-19) and ChildrenSUNDAY, FEBRUARY 23, 2020
- Frequently Asked Questions and Answers: Coronavirus Disease 2019 (COVID-19) and PregnancyFRIDAY, FEBRUARY 21, 2020
- Stigma Related to COVID-19FRIDAY, FEBRUARY 21, 2020
- Resources for State, Local, Territorial and Tribal Health DepartmentsTHURSDAY, FEBRUARY 20, 2020
- Interim Guidance for Collection and Submission of Postmortem Specimens from Deceased Persons Under Investigation (PUI) for COVID-19WEDNESDAY, FEBRUARY 19, 2020
school marm
Senior Member
I did my Sam's run today. Could not tell that anyone there was shopping for the virus. Saw only ONE lady wearing a mask--Asian. Kept my distance from her. All shelves well-stocked, no shortages. Did get one of the last packages of my favorite TP (Scott's) but plenty of other brands still there. Absolutely FURIOUS to discover you can no longer buy those great big cardboard boxes of Carnation powdered milk! They apparently no longer make / sell it! I am furious with myself that I recently donated all my old Y2K supply of powedered milk (something like 15 boxes) to a food donation center---I figured it was old and I'd just get some new at Sam's. Didn't know they had STOPPED MAKING IT except in little bitty bags or small cans!!! Even on the internet couldn't find it. Finally bought two BAGS (plastic BAGS---am concerned how well those are sealed and will last) at Kroger. ANYONE KNOW WHERE I can get LARGE boxes of powdered milk anymore?
A case of twelve 28-oz bags runs $62.75. If you have a Home Storage Center near you and can purchase in person, it's substantially less.
So I went looking for the percentage of people who smoke in a variety of nations who have been hit with the WuFlu. Interesting. And not necessarily comforting.
An estimated 14 percent of adults in the U.S., or 34.3 million people, smoked cigarettes in 2017, down from 15.5 percent in 2016, according to the CDC.Nov 8, 2018
CDC says smoking rates fall to record low in US - CNBC.com
www.cnbc.com › 2018/11/08 › cdc-says-smoking-rates-fall-to-record-lo.
About 20% of the adult male and 4.5% of the adult female population smoke tobacco (12 million smokers according to some estimates). 60,000 Iranians die directly or indirectly due to smoking every year (2008). Smoking is responsible for 25% of deaths in the country.
Smoking in Iran - Wikipedia
en.wikipedia.org › wiki › Smoking_in_Iran
??? Different sources for Iran, different numbers, and different years. Shrug.
We recently showed that the prevalence rate of current and daily cigarette smoking in Iran is correspondingly 12.5% (23.4% males and 1.4% females; burden: 6.1 million) and 11.3% (21.4 males and 1.4 females; burden: 5.6 million).Feb 29, 2012
Cigarette Smoking in Iran - NCBI
www.ncbi.nlm.nih.gov › pmc › articles › PMC3481682
China has the largest smoking population in the world, with around 316 million adult smokers, and accounts for nearly one-third (30%) of smokers and 40% of tobacco consumption worldwide (4). In 2015, smoking prevalence was 27.7% (52.1% among men and 2.7% among women) (5).Mar 12, 2019
Tobacco and the lung cancer epidemic in China - NCBI - NIH
www.ncbi.nlm.nih.gov › pmc › articles › PMC6546632
The rates are age-standardized. Italy smoking rate for 2016 was 23.70%, a 0.1% decline from 2015. Italy smoking rate for 2015 was 23.80%, a 0.3% decline from 2014. Italy smoking rate for 2014 was 24.10%, a 0% increase from 2013.
Italy Smoking Rate 2000-2020 | MacroTrends
www.macrotrends.net › countries › ITA › italy › smoking-rate-statistics
In 2015, the adult smoking rate was 19.3%, 29.7% of Japanese men and 9.7% of Japanese women. This is the lowest recorded figure since Japan Tobacco began surveying in 1965. As of July 2016, just over 20,000,000 people smoked in Japan, though the nation remained one of the world's largest tobacco markets.
Smoking in Japan - Wikipedia
en.wikipedia.org › wiki › Smoking_in_Japan
Smoking in South Korea is similar to other developed countries in the OECD, with a daily smoking rate of 19.9% in 2013 compared to 20.9% in Germany and 19.3% in Japan. However, male smoking is among the highest at 36.2% while female smoking by far the lowest at 4.3%.
Smoking in South Korea - Wikipedia
en.wikipedia.org › wiki › Smoking_in_South_Korea
According to a 2013 micro-census survey, 24.5% of the German population aged fifteen years and over are smokers (29% of men, 20% of women). Among the 18–25 age group, 35.2% are smokers.
Smoking in Germany - Wikipedia
en.wikipedia.org › wiki › Smoking_in_Germany
An estimated 14 percent of adults in the U.S., or 34.3 million people, smoked cigarettes in 2017, down from 15.5 percent in 2016, according to the CDC.Nov 8, 2018
CDC says smoking rates fall to record low in US - CNBC.com
www.cnbc.com › 2018/11/08 › cdc-says-smoking-rates-fall-to-record-lo.
About 20% of the adult male and 4.5% of the adult female population smoke tobacco (12 million smokers according to some estimates). 60,000 Iranians die directly or indirectly due to smoking every year (2008). Smoking is responsible for 25% of deaths in the country.
Smoking in Iran - Wikipedia
en.wikipedia.org › wiki › Smoking_in_Iran
??? Different sources for Iran, different numbers, and different years. Shrug.
We recently showed that the prevalence rate of current and daily cigarette smoking in Iran is correspondingly 12.5% (23.4% males and 1.4% females; burden: 6.1 million) and 11.3% (21.4 males and 1.4 females; burden: 5.6 million).Feb 29, 2012
Cigarette Smoking in Iran - NCBI
www.ncbi.nlm.nih.gov › pmc › articles › PMC3481682
China has the largest smoking population in the world, with around 316 million adult smokers, and accounts for nearly one-third (30%) of smokers and 40% of tobacco consumption worldwide (4). In 2015, smoking prevalence was 27.7% (52.1% among men and 2.7% among women) (5).Mar 12, 2019
Tobacco and the lung cancer epidemic in China - NCBI - NIH
www.ncbi.nlm.nih.gov › pmc › articles › PMC6546632
The rates are age-standardized. Italy smoking rate for 2016 was 23.70%, a 0.1% decline from 2015. Italy smoking rate for 2015 was 23.80%, a 0.3% decline from 2014. Italy smoking rate for 2014 was 24.10%, a 0% increase from 2013.
Italy Smoking Rate 2000-2020 | MacroTrends
www.macrotrends.net › countries › ITA › italy › smoking-rate-statistics
In 2015, the adult smoking rate was 19.3%, 29.7% of Japanese men and 9.7% of Japanese women. This is the lowest recorded figure since Japan Tobacco began surveying in 1965. As of July 2016, just over 20,000,000 people smoked in Japan, though the nation remained one of the world's largest tobacco markets.
Smoking in Japan - Wikipedia
en.wikipedia.org › wiki › Smoking_in_Japan
Smoking in South Korea is similar to other developed countries in the OECD, with a daily smoking rate of 19.9% in 2013 compared to 20.9% in Germany and 19.3% in Japan. However, male smoking is among the highest at 36.2% while female smoking by far the lowest at 4.3%.
Smoking in South Korea - Wikipedia
en.wikipedia.org › wiki › Smoking_in_South_Korea
According to a 2013 micro-census survey, 24.5% of the German population aged fifteen years and over are smokers (29% of men, 20% of women). Among the 18–25 age group, 35.2% are smokers.
Smoking in Germany - Wikipedia
en.wikipedia.org › wiki › Smoking_in_Germany
marsh
On TB every waking moment
Decoding evolution and transmissions of novel pneumonia coronavirus using the whole genomic data
Submit Time: 2020-02-21Author: Yu, Wen-Bin 1,2 ; Tang, Guang-Da 3,4 ; Zhang, Li 5 ; Corlett, Richard T. 1.2 ;Institute: 1.Center for Integrative Conservation, Xishuangbanna Tropical Botanical Garden, Chinese Academy of Sciences, Mengla, Yunnan 666303, China; 2.Center of Conservation Biology, Core Botanical Gardens, Chinese Academy of Sciences, Mengla, Yunnan 666303, China; 3.Henry Fok College of Biology and Agriculture, Shaoguan University, Shaoguan 512005, China; 4.College of Forestry and Landscape Architecture, South China Agricultural University, Guangzhou 510642, China; 5.Chinese Institute for Brain Research, Beijing 102206, China;
更多0
Abstracts
Submit Time: 2020-02-21Author: Yu, Wen-Bin 1,2 ; Tang, Guang-Da 3,4 ; Zhang, Li 5 ; Corlett, Richard T. 1.2 ;Institute: 1.Center for Integrative Conservation, Xishuangbanna Tropical Botanical Garden, Chinese Academy of Sciences, Mengla, Yunnan 666303, China; 2.Center of Conservation Biology, Core Botanical Gardens, Chinese Academy of Sciences, Mengla, Yunnan 666303, China; 3.Henry Fok College of Biology and Agriculture, Shaoguan University, Shaoguan 512005, China; 4.College of Forestry and Landscape Architecture, South China Agricultural University, Guangzhou 510642, China; 5.Chinese Institute for Brain Research, Beijing 102206, China;
更多0
Abstracts
| Background. The outbreak of COVID-19 started in mid-December 2019 in Wuhan, Central China. Up to February 18, 2020, SARS-CoV-2 has infected more than 70,000 people in China, and another 25 countries across five continents. In this study, we used 93 complete genomes of SARS-CoV-2 from the GISAID EpiFluTM database to decode the evolution and human-to-human transmissions of SARS-CoV-2 in the recent two months. Methods. Alignment of coding-regions was conducted haplotype analyses using DnaSP. Substitution sites were analyzed in codon. Evolutionary analysis of haplotypes used NETWORK. Population size changes were estimated using both DnaSP and Arlequin. Expansion date of population size was calculated based on the expansion parameter tau (τ) using the formula t=τ/2u. Findings. Eight coding-regions have 120 substitution sites, including 79 non-synonymous and 40 synonymous substitutions. Forty-two non-synonymous substitutions changed the biochemical property of amino acids. No evident combination was found. Fifty-eight haplotypes were classified as five groups, and 31 haplotypes were found in samples from both China and other countries, respectively. The rooted network suggested H13 and H35 to be ancestral haplotypes, and H1 (and its descendent haplotypes including all samples from the Hua Nan market) was derived H3 haplotype. Population size of SARS-CoV-2 were estimated to have a recent expansion on 6 January 2020, and an early expansion on 8 December 2019. Interpretation. Genomic variations of SARS-CoV-2 are still low in comparisons with published genomes of SARS-CoV and MERS-CoV. Phyloepidemiologic analyses indicated the SARS-CoV-2 source at the Hua Nan market should be imported from other places. The crowded market boosted SARS-CoV-2 rapid circulations in the market and spread it to the whole city in early December 2019. Furthermore, phyloepidemiologic approaches have recovered specific direction of human-to-human transmissions, and the import sources of international infectious cases. |
marsh
On TB every waking moment

The Coronavirus Disease 2019 (COVID-19) Outbreak in China—Summary of a China CDC Report
This Viewpoint summarizes key epidemiologic and clinical findings from all cases of coronavirus disease 2019 (COVID-19) reported through February 11, 2020, in mainland China, and case trends in response to government attempts to control and contain the infection.
 jamanetwork.com
jamanetwork.com
Viewpoint
February 24, 2020
Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in ChinaSummary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention
Zunyou Wu, MD, PhD1; Jennifer M. McGoogan, PhD1
Author Affiliations Article Information
JAMA. Published online February 24, 2020. doi:10.1001/jama.2020.2648
COVID-19 Resource Center
The Chinese Center for Disease Control and Prevention recently published the largest case series to date of coronavirus disease 2019 (COVID-19) in mainland China (72 314 cases, updated through February 11, 2020).1 This Viewpoint summarizes key findings from this report and discusses emerging understanding of and lessons from the COVID-19 epidemic.
Epidemiologic Characteristics of the COVID-19 Outbreak
Among a total of 72 314 case records (Box), 44 672 were classified as confirmed cases of COVID-19 (62%; diagnosis based on positive viral nucleic acid test result on throat swab samples), 16 186 as suspected cases (22%; diagnosis based on symptoms and exposures only, no test was performed because testing capacity is insufficient to meet current needs), 10 567 as clinically diagnosed cases (15%; this designation is being used in Hubei Province only; in these cases, no test was performed but diagnosis was made based on symptoms, exposures, and presence of lung imaging features consistent with coronavirus pneumonia), and 889 as asymptomatic cases (1%; diagnosis by positive viral nucleic acid test result but lacking typical symptoms including fever, dry cough, and fatigue).1
Box.
Key Findings From the Chinese Center for Disease Control and Prevention Report
- 72 314 Cases (as of February 11, 2020)
- Confirmed cases: 44 672 (62%)
- Suspected cases: 16 186 (22%)
- Diagnosed cases: 10 567 (15%)
- Asymptomatic cases: 889 (1%)
- Age distribution (N = 44 672)
- ≥80 years: 3% (1408 cases)
- 30-79 years: 87% (38 680 cases)
- 20-29 years: 8% (3619 cases)
- 10-19 years: 1% (549 cases)
- <10 years: 1% (416 cases)
- Spectrum of disease (N = 44 415)
- Mild: 81% (36 160 cases)
- Severe: 14% (6168 cases)
- Critical: 5% (2087 cases)
- Case-fatality rate
- 2.3% (1023 of 44 672 confirmed cases)
- 14.8% in patients aged ≥80 years (208 of 1408)
- 8.0% in patients aged 70-79 years (312 of 3918)
- 49.0% in critical cases (1023 of 2087)
- Health care personnel infected
- 3.8% (1716 of 44 672)
- 63% in Wuhan (1080 of 1716)
- 14.8% cases classified as severe or critical (247 of 1668)
- 5 deaths
The overall case-fatality rate (CFR) was 2.3% (1023 deaths among 44 672 confirmed cases). No deaths occurred in the group aged 9 years and younger, but cases in those aged 70 to 79 years had an 8.0% CFR and cases in those aged 80 years and older had a 14.8% CFR. No deaths were reported among mild and severe cases. The CFR was 49.0% among critical cases. CFR was elevated among those with preexisting comorbid conditions—10.5% for cardiovascular disease, 7.3% for diabetes, 6.3% for chronic respiratory disease, 6.0% for hypertension, and 5.6% for cancer. Among the 44 672 cases, a total of 1716 were health workers (3.8%), 1080 of whom were in Wuhan (63%). Overall, 14.8% of confirmed cases among health workers were classified as severe or critical and 5 deaths were observed.1
COVID-19 rapidly spread from a single city to the entire country in just 30 days. The sheer speed of both the geographical expansion and the sudden increase in numbers of cases surprised and quickly overwhelmed health and public health services in China, particularly in Wuhan City and Hubei Province. Epidemic curves reflect what may be a mixed outbreak pattern, with early cases suggestive of a continuous common source, potentially zoonotic spillover at Huanan Seafood Wholesale Market, and later cases suggestive of a propagated source as the virus began to be transmitted from person to person (Figure 1).1
Figure 1.
Download
")
Epidemic Curve of the Confirmed Cases of Coronavirus Disease 2019 (COVID-19)
Daily numbers of confirmed cases are plotted by date of onset of symptoms (blue) and by date of diagnosis (orange). Because, on retrospective investigation, so few cases experienced illness in December, these cases are shown in the inset. The difference between the cases by date of symptom onset curve (blue) and the cases by date of diagnosis curve (orange) illustrates lag time between the start of illness and diagnosis of COVID-19 by viral nucleic acid testing. The graph's x-axis (dates from December 8, 2019, to February 11, 2020) is also used as a timeline of major milestones in the epidemic response. The first few cases of pneumonia of unknown etiology are shown in blue boxes on December 26 (n = 4) and 28-29 (n = 3). Most other cases that experienced onset of symptoms in December were only discovered when retrospectively investigated. Major epidemic response actions taken by the Chinese government are shown in brown boxes. The normally scheduled Lunar New Year national holiday is shown in light yellow, whereas the extended holiday during which attendance at school and work was prohibited (except for critical personnel such as health workers and police) is shown in dark yellow. This figure was adapted with permission.1 CDC indicates Chinese Center for Disease Control and Prevention; HICWM, Hubei Integrated Chinese and Western Medicine; 2019-nCoV, 2019 novel coronavirus; WHO, World Health Organization.
( Continued on website)
Roundaben--
Given your conversation above w Trivium Pursuit--and the Twitter video from the Chinese lady CONFIRMING what we'd already heard about still-alive people being creamted because when they reached the point of needing assistance to breathe the hospital had NOTHING to help them breathe--no respirators, no oxygen machines----
I have a question for you.
I'm in my 60's, have had pneumonia 4 times (first time in just my 20's, twice during my 30's, last time was last year - March--and I thought I'd NEVER get over it)---PLUS I am allergic to cephalosporins, macrobid, sulfa (VERY allergic to that) and react very badly (toxic, not allergic) to floxacins. Only antibiotics left I can take are the cillins (oddly enough NOT allergic to those, though I am to the cephalosporins), doxycycline, erythromycin, etc. I also have a family history of heart troubles, though personally have experienced nothing worse than episodes of irregular heartbeat (usually from getting too tired, not drinking enough water, too low on potassium, etc.). Plus I'm about 40 pounds overweight & out of shape.
What I am worried about is what happens to my special-needs sons (young and healthy) if something happens to me.
So while I can deal with the "flu" if it just STAYS flu, I am worried about it turning into pneumonia, given how many antibiotics I'm allergic to. I also am worried about an over-loaded hospital system where I can't go in daily to my doctor's for albuterol inhalation therapy (which she did to keep me out of the hospital last year). (I do have an aerosol inhalation machine at home and some leftover albuterol doses, if they're still good after a year).
Now here's my question.
I was looking into the possibility--in case of mass quarantines being declared here OR hospitals becoming overloaded or both---of getting an oxygen concentrator. However, have learned---you can't just go out and buy one of those without a doctor's prescription, you can't legally sell (and thus, can't buy used) a used one unless "all original materials" come with it, and over-using or improperly using oxygen can be dangerous, even fatal.
Given that---weighing one thing against another---is it a wise thing for us to "consider" trying to lay hands on an oxygen concentrator---or could we be doing ourselves more harm than good by having one but not using it right? (too soon, too long, at the improper time where it can CAUSE respiratory distress instead of curing it)--????
....Or should I be glad I've updated my will, just "do the best I can"---and pray? (iow, I'm screwed)
I'm going to be very careful here. I understand your concerns and I'll do my best to answer your questions as I can.
First, and this may seem to be insensitive----If what was said was done about burning patients alive is true it is an indictment of the inhumanity of the chinese political system and culture. We have little control of how we are born and many times less control of how we die. That was taken away from these people and imposed by a system that sees human life as meaningless. I would not allow that to happen to me or mine.
Now, your medical situation. Without examining you I cannot give you any definitive answers. I would recommend that you take you concerns to your physician. They know you and have successfully treated you in the past. They know your allergy history and, more importantly, can prescribe you rounds of antibiotics that are appropriate for prophylaxis as well as treatment of likely pathogens. Its not an unreasonable discussion to have with them.
I would also express your concerns about prior breathing problems in the face of an oncoming pandemic. I don't think that it would be unreasonable to ask for refills on the albuterol nebulizer, new masks and kits, or asking about the ability to use supplemental oxygen if you did become sick. Your doc could prescribe those things for you, especially if there are large numbers of people at the hospital it would be helpful for you to not go in just for treatment and risk exposure for conditions that you could manage at home with the correctly prescribed equipment and medications. Oxygen could be very important for you with your past history. I would consider seriously talking to them.
Finally, there are some steps I would recommend. DO have a living will, powers of attorney, and all of the documents drawn up to assure that your sons are cared for. Have a system where people you know can come to check on you and them, and that you can trust to check on you if you are unable to request help so that your sons are not left unattended. Put your thoughs in energy into preparing for the worst, hoping for the best, and never giving up.
And talk to your doc about the meds, nebulizers, and oxygen.
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
 www.zerohedge.com
www.zerohedge.com

by Tyler Durden
Tue, 02/25/2020 - 21:45
Unprepared countries across the Middle East are scrambling to respond as they've begun recording more and more coronavirus cases.
While official government figures across the region likely fall short of the true number — for example hard hit Iran may have already seen 50 deaths according to one lawmaker in the city of Qom despite the Health Ministry denying this high figure and confirming only 12 deaths to date — it's deeply alarming that Covid-19 has been confirmed in multiple corners of the Middle East, from Egypt to the Gulf to Iran.

Notice also that the United Arab Emirates now has at least 13 confirmed cases, in a worrisome sign in could hit the gulf region hard, given also it's a major international transport hub straddling east Asia and the West.
The WHO is especially concerned of an outbreak among refugee populations in war-torn regions of Iraq and Syria.
"Health officials in both countries remain under-equipped to deal with such a a reality that seems more possible with each passing day," the report added."Refugees and internally displaced populations across Iraq and Syria have been identified as the most vulnerable groups in the region, should the spread of the virus become a pandemic," The Guardian reports of recent statements.
Sprawling and densely packed "tent cities" of refugees along the border areas of Syria remain the most vulnerable.
 Refugee camp in northwest Syria, via the AP.
Refugee camp in northwest Syria, via the AP.Official government numbers of infected in the region are as follows:
- Bahrain (17 cases)
- Egypt (1 case)
- Iran (61 cases)
- Iraq (5 cases)
- Israel (2 cases)
- Kuwait (3 cases)
- Lebanon (1 case)
- Oman (4 cases)
- UAE (13 cases)
The below includes excerpts of Middle East Eye's brief summary report on confirmed coronavirus cases in each country.
* * *
Bahrain (17 cases)
Bahrain's health ministry announced on 25 February that a total of 17 people have been infected with the coronavirus.
The ministry reported its first case of the coronavirus on 24 February after a "citizen arriving from Iran was suspected of having contracted the virus based on emerging symptoms"...
Egypt (1 case)
The WHO confirmed on 19 February that a man identified a week earlier was recovering and no longer a carrier of the illness, but would remain in quarantine for the mandated 14 days.
Iran (61 cases, 16 dead)
Iran is the worst-hit country outside of China, with at least 16 people dead due to the coronavirus. Several countries in the region confirmed their first patients had all previously been in Iran.
The country's deputy health minister, tasked with heading the country's response, was also infected by the virus, a health ministry announcement confirmed on Tuesday 25 February...
On 24 February, an Iranian MP accused the government of "lying" about the extent of the virus's spread in Iran, claiming 50 people have been killed by it in the holy city of Qom alone.
Iraq (5 cases)
Iraq confirmed four new cases of the coronavirus on 25 February in an Iraqi family returning from Iran to the city of Kirkuk.
Baghdad reported its first case of the coronavirus on 24 February. Health officials said the patient was an Iranian theology student living in the southern city of Najaf.
All students studying at the same religious seminary were quarantined, while one of the city's most important religious sites was temporarily closed to pilgrims while it was disinfected.
Israel (2 cases)
An Israeli woman tested positive for the virus after returning from a heavily affected cruise ship, Israel announced on 21 February.
The country later sent 180 South Korean tourists back home and closed travel to and from South Korea. According to Israeli media, the government is considering quarantining another 200 South Koreans at a military base.
Kuwait (3 cases)
The Kuwaiti health ministry reported its first cases of coronavirus on 24 February.
In a statement posted on Twitter, the ministry said: "Tests conducted on those coming from the Iranian holy city of Mashhad showed there were three confirmed cases of the coronavirus (COVID-19)."...
Lebanon (1 case)
The first confirmed case in Lebanon involved a 45-year-old woman who had travelled from Iran and was quarantined.
She had arrived on a plane from the Iranian city of Qom, where authorities have said Iran's outbreak started.
Oman (4 cases)
Oman reported two more cases of coronavirus from individuals who had just travelled to Iran, according to the country's health ministry Twitter account.
The health ministry reported the first two cases of coronavirus infections in the country on 24 February, Oman TV said.
The two Omani women diagnosed with the illness had visited Iran, it said. They are in a stable condition...
UAE (13 cases)
The UAE banned all travel to Iran and Thailand over fears about the spread of the virus, state news agency WAM reported on 24 February.
It recorded the first of its 13 cases when four members of a Chinese family were diagnosed on 28 January.
jward
passin' thru
I see that the olympics are moving right along- they were definitely on a week ago, and now, all but cancelled...

Reuters
@Reuters
·
27m
Dentsu's shares slide to seven year lows on Olympics cancellation fears https://reut.rs/2HUGmBX
Reuters
@Reuters
·
27m
Dentsu's shares slide to seven year lows on Olympics cancellation fears https://reut.rs/2HUGmBX
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
How Many Cases Of Covid-19 Will It Take For You To Decide Not To Frequent Public Places?
Tue, 02/25/2020 - 20:05
Authored by Charles Hugh Smith via OfTwoMinds blog,
As empty streets and shelves attest, people taking charge of risk has dire economic consequences.
How many cases of Covid-19 in your community will it take for you to decide not to frequent public places such as cafes, restaurants, theaters, concerts, etc? How many cases in your community will it take for you to decide not to take public transit, Uber/Lyft rides, etc.? How many cases in your community will it take for you to limit going to supermarkets and ask your boss to work at home?

One of the most unexamined aspect of the Covid-19 pandemic is the human psychology of risk assessment and fear. The default human response to novel threats such as the Covid-19 virus is denial and abstraction: it can't happen here, it won't happen to me, it's no big deal, etc.
This careless denial of danger and urgency characterized the official response in China before the epidemic exploded and it characterizes the lackadaisical sloppiness of official response in the U.S.: few facilities have test kits, thousands of people who arrived on U.S. soil on direct flights from Wuhan have not been tested, confirmed carriers have been placed on flights with uninfected people, and the city of Costa Mesa, CA had to file a lawsuit to stop federal agencies from transferring confirmed carriers to dilapidated facilities that are incompatible with thorough quarantine protocols.
This lackadaisical sloppiness didn't hinder the spread of the virus in China and it won't hinder it in the U.S. That means each of us will eventually have to make our own risk assessments and decide to modify our routines and behaviors or not.
Hence the question: what's your red line number? Do you stop going out to public places and gatherings when there's ten confirmed cases in your community, or is your red line number 50 cases? Or is it 100?
For many people, even a handful of cases will be a tremendous shock because they were unrealistically confident that it can't happen here. The realization that the virus is active locally and can be spread by people who don't have any symptoms shatters the comfortable complacency and introduces a chilling reality: what was an abstraction is now real.
Human psychology is exquisitely attuned to risk once it moves from abstraction to reality. Why take a chance unless absolutely necessary? For many people, the first handful of local cases will be enough to cancel all exposure to optional public gatherings: cafes, bistros, theaters, concerts, etc.
Many others will decide to forego public transit, taxis and Uber/Lyft rides because who knows if the previous fare was an asymptomatic carrier?
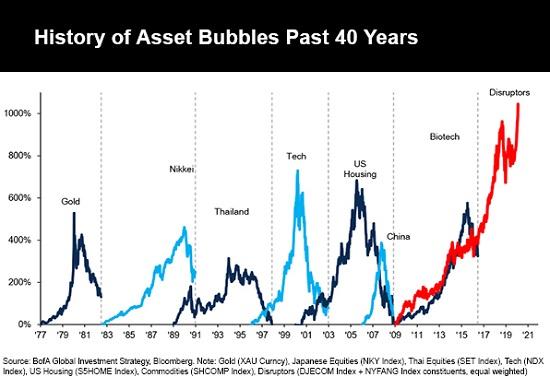
If you doubt this impulse to over-reaction once abstraction gives way to reality, look at how quickly market shelves are stripped in virus-affected areas. Once we understand what rationalists might declare over-reaction is merely prudence when faced with difficult-to-assess dangers, we realize that there's a bubble not just in the stock market and Big Tech but in complacency.
Once a consequential number of people decide to avoid public places and gatherings, streets become empty and all the businesses that depend on optional public mixing--cafes, bistros, restaurants, theaters, music venues, stadiums, etc. etc. etc.-- dry up and blow away, even if officials maintain their careless denial of danger and urgency.
All the jobs in this vast service sector will suddenly be at risk, along with the survival of thousands of small businesses, many of which do not have the resources to survive weeks, much less months, of a sharp decline in business.
All the official reassurances won't be worth a bucket of warm spit. After being assured the risk of the virus spreading in North America was "low," the arrival of the virus will destroy trust in official assurances. People will awaken to the need to control their own risk factors themselves. And as empty streets and shelves attest, people taking charge of risk has dire economic consequences.
Scarletbreasted
Galloping geriatric
No wonder the high numbers of co-morbidities in China...........look at their Lung Cancer stats (Derived from Pinecone's source for data a few posts above)
China is in the midst of a lung cancer epidemic on an unprecedented scale. In 2015, there were an estimated 733,000 new lung cancer cases (17% of total cancer incidence) and 610,000 deaths (21.7% of total cancer mortality) in China. Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer mortality in China. While 70% of lung cancer cases occur in men (1), among women lung cancer is second to breast cancer in frequency of diagnosis and remains the leading cause of cancer death.
As lung cancer incidence and mortality have been decreasing in most high-income countries, age-standardized lung cancer incidence and mortality rates in China have been steadily increasing since 1990 (2,3).
The most substantial factor driving recent lung cancer trends in China is tobacco smoke exposure. China has the largest smoking population in the world, with around 316 million adult smokers, and accounts for nearly one-third (30%) of smokers and 40% of tobacco consumption worldwide (4). In 2015, smoking prevalence was 27.7% (52.1% among men and 2.7% among women) (5). Although the prevalence of smoking among women in China is relatively low, exposure to secondhand smoke is high.
China has taken some important steps for tobacco control, including ratifying the World Health Organization Framework Convention on Tobacco Control (FCTC) and implementing comprehensive smoke free workplace laws in a number of cities. However, smoking prevalence has remained relatively stable over the past decade (6). At the same time, new developments, such as the introduction of alternative nicotine delivery systems (ANDS) and rising disparities in tobacco use, pose new challenges for the future.
This paper reviews trends in lung cancer and tobacco use in China, along with progress in tobacco control efforts. Overall, tobacco smoking causes over 1 million deaths annually in China and this number is projected to rise to 2 million in 2030 and 3 million by 2050 (7). While tobacco smoke exposure is associated with several cancers as well as cardiovascular and lung disease, the strength of the association with lung cancer and the high lung cancer burden in China warrant a particular focus on lung cancer.
sb
China is in the midst of a lung cancer epidemic on an unprecedented scale. In 2015, there were an estimated 733,000 new lung cancer cases (17% of total cancer incidence) and 610,000 deaths (21.7% of total cancer mortality) in China. Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer mortality in China. While 70% of lung cancer cases occur in men (1), among women lung cancer is second to breast cancer in frequency of diagnosis and remains the leading cause of cancer death.
As lung cancer incidence and mortality have been decreasing in most high-income countries, age-standardized lung cancer incidence and mortality rates in China have been steadily increasing since 1990 (2,3).
The most substantial factor driving recent lung cancer trends in China is tobacco smoke exposure. China has the largest smoking population in the world, with around 316 million adult smokers, and accounts for nearly one-third (30%) of smokers and 40% of tobacco consumption worldwide (4). In 2015, smoking prevalence was 27.7% (52.1% among men and 2.7% among women) (5). Although the prevalence of smoking among women in China is relatively low, exposure to secondhand smoke is high.
China has taken some important steps for tobacco control, including ratifying the World Health Organization Framework Convention on Tobacco Control (FCTC) and implementing comprehensive smoke free workplace laws in a number of cities. However, smoking prevalence has remained relatively stable over the past decade (6). At the same time, new developments, such as the introduction of alternative nicotine delivery systems (ANDS) and rising disparities in tobacco use, pose new challenges for the future.
This paper reviews trends in lung cancer and tobacco use in China, along with progress in tobacco control efforts. Overall, tobacco smoking causes over 1 million deaths annually in China and this number is projected to rise to 2 million in 2030 and 3 million by 2050 (7). While tobacco smoke exposure is associated with several cancers as well as cardiovascular and lung disease, the strength of the association with lung cancer and the high lung cancer burden in China warrant a particular focus on lung cancer.
sb
Countrymouse
Country exile in the city
Have you looked on Amazon? We bought a 2lb bag of powdered milk there, and it was quite reasonable.
When my husband looked, all he could find were 10 oz packages---I know the large Carnation boxes I used to get must have weighed 5 pounds at least! Doesn't anyone still make them that big?
Rucus Sunday
Veteran Member
Visited 2 stores today in PNW, Safeway & Fred Meyer. No sign of any prepping, in fact relatively light shopping traffic. I had the "pick of the litter" in terms of what I wanted, shelves neatly lined with row upon row of canned meats, soups, veg, fruit, etc.
Uhhmmm...
Veteran Member
With regard to the CDC recently announcing the coming pandemic... I regard their advice just as I do that of the financial nabobs...
When they say strong buy, it is time to look at the fundamentals.
When they say buy, it is time to hold.
When they say hold, it is time to sell.
When they say sell, you are eff'ed.
When they say strong buy, it is time to look at the fundamentals.
When they say buy, it is time to hold.
When they say hold, it is time to sell.
When they say sell, you are eff'ed.
Countrymouse
Country exile in the city
Here is a posting by
CDC Warns on Coronavirus: "It’s inevitable...” Here's How To Prepare
concerning the CDC video on the out break of the Virus....
The video has been scrubbed from the internet....
There is a lot more to this COVID-10 Virus than any government and our government agencies are releasing....
Prepare accordingly....
Prepare now for it is out to the American public...
Texican....
--------------------------------------------------------------
CDC Warns on Coronavirus: “It’s inevitable…” Here’s How To Prepare
As of today, the total number of accumulated COVID-19 infections nationwide is 77,658, with 2,663 deaths. With this rapidly evolving outbreak, the CDC has done its best to stay in control of the rhetoric of keeping the public informed. Their main focus was to stay cautiously alert and keep the public calm, but as of […]
TESS PENNINGTON
As of today, the total number of accumulated COVID-19 infections nationwide is 77,658, with 2,663 deaths.
With this rapidly evolving outbreak, the CDC has done its best to stay in control of the rhetoric of keeping the public informed. Their main focus was to stay cautiously alert and keep the public calm, but as of today, they have significantly shifted their official statement and there is no denying the fact that coronavirus will come to communities in the U.S.
In another article, “The CDC said the agency would be shifting strategies and using a dual approach. Health officials still plan to try to contain the spread and slow down the spread of the virus into the United States. At the same time, health officials are now urging businesses, health-care facilities, and even schools to plan now for ways to limit the impact of illness when it spreads in the community.”
Without a tested tried-and-true vaccine, it is just a matter of time before the same things that are happening elsewhere start happening here. And with that, also comes the panic from those who are underprepared. The following are six key warning signs you should be looking for. The following information was taken from The Prepper’s Blueprint:
When these events come to pass or you see these signals, you should strongly consider implementing a self-quarantine lockdown:
If any of these signs begin to appear around you, it’s time to seriously consider distancing yourself from society, and especially highly dense venues like retail stores, sporting events or schools.
- Emergency officials say they have the situation under control, but more cases continue to pop up.
- Local and state governments officially declare an emergency.
- Cases have been identified at your local hospital or at schools in your general vicinity.
- The general public begins to panic and store shelves start running out of key supplies like food and bottled water.
- Looting and lawlessness occur within the local community.
- The virus breaches a 50-mile radius surrounding your home or town.
You Have an Opportunity To Get Prepared
In our last article, 9 Ways to Prepare for COVID-19, we mentioned there is a small block of time to get supplies in order before this virus winds up knocking on your door. Moreover, to be prepared for an infectious outbreak, home quarantine procedures and avoiding contact with the outside will need to be your focus. Therefore, you need to focus on a wide range of preparedness subjects in order to get fully prepared and you are running out of time.
For an introduction into pandemic preparedness and a list of preparedness items to buy, click here.
Here’s an important factor to consider: You want to have all supplies and a plan in place before the virus spreads out of control and before government officials force mandatory quarantines. Once the signs start to appear, it may already be too late to start stockpiling supplies because panic-buying will be the order of the day. We’ve already seen this with major internet suppliers of medical gear, who report that their inventories have been nearly cleaned out. The same will happen on a local level.
In this type of disaster, you need to prepare for the likelihood of living in an off-grid setting with the supplies in your home for at least a month. That’s the bare minimum! Here is a basic starter list compiled from portions of The Prepper’s Blueprint. If you are serious about protecting yourself from a potential pandemic there is a lot to do, but the following guidelines can fast-track your preparedness and contingency plans.
Bug In Supplies
Water – Have a short term water supply. Emergency organizations suggest 1 gallon per person for 30 days. If one goes by this suggestion, to have 1 gallon per person per day, a family of 5 will need 35 gallons of water per week. Further, it would be ideal to have some tools to treat water such as a portable filtration system, chemical treatment tablets, etc., as well as a portable filtration system for your bug out bags. To learn the different methods of purifying water, click here.
Note: As a backup plan, consider investing in manual water pumps, tarps, rain gutters for the home to collect rainwater and condensation from the ground, trees, and bushes. This could save your life!
Food – Have a 30-day supply of shelf-stable foods. You need to assume that electricity could go out, therefore look to foods that do not require refrigeration. To see how much your family would need, click here. Create a menu based around your shelf-stable foods to ensure you have enough food to feed your family. Your menu should be realistic in the sense that it will provide your body with the necessary energy needs. This chart can help in researching caloric needs based on gender and age. At the very least, plan for 1200 calories per meal. Keep healthy whole grains in mind when adding carbohydrates to your larder. Above all, ensure the foods you choose to promote health.
Health – First and foremost, mimic what the healthcare professionals are doing. If the CDC is getting ready and recommending healthcare professionals to have protective equipment or PPE, then you should too! At the very least, here are some items they are recommending to healthcare professionals: Disposable gowns, gloves, NIOSH-certified disposable N95 respirator, eye protection. Further, have a supply of medicines for respiratory illnesses, health-boosting vitamins, immune-boosting teas (try these). Get a full list of pandemic supplies here.
Sanitation – In a pandemic, everyone will fear going to their jobs and all forms of normal life will be on hold. This includes your trash pickups. Have a basic sanitation kit and prepare for the fact that toilets won’t flush, trash won’t be collected and you will be on your own. When sanitary conditions are not up to par, there is an increase in diseases such as cholera, typhoid, and diphtheria. Typically, women and children are the most affected by poor sanitary conditions. Women’s personal hygiene is essential to her health and should be considered a priority in your sanitation preparedness measures. Taking proper precautions and stocking up on sanitary items will help eliminate most issues regarding poor sanitation.
Alternative power – Disasters of any kind cause grid-down scenarios. In this case, if a pandemic ensues, people are not going to risk exposing themselves to a deadly contagion just so the public has their electricity. Prepare to live in an off-grid environment and invest in alternative means of power and invest in rechargeable batteries, solar battery chargers, generators, ample supplies of fuel and even a siphon for fuel. As well, if cold weather threatens the area where you live, have ample firewood and matches or a way to start a fire.
Communication – You can’t cut yourself off from the world, especially in a disaster. Our normal forms of communication – television, cell phones, landlines may not be available following a disaster. Therefore, you will need alternative forms of communication to communicate with neighbors, loved ones or to learn what is happening in your community. Having police scanners, radios, Ham radios to communicate to the outside world will give you a huge advantage in survival and security.
Security – Never underestimate the desperation of those who are unprepared or ill-equipped to survive. When one’s needs are not met, there is nothing they won’t do. Bugging in will require more planning and security on your part. Although living in an urban center may be the most difficult in terms of survival, those that live on the city’s outskirts and suburban areas will not be without their own set of challenges.
Considering that the majority of the U.S. population is centered in 146 of the country’s 3000 counties, chances are most of us live in urban areas, and special attention must be placed on security. We’ve read enough survival stories to know that drug addicts, released prisoners, those with mental illnesses and the unprepared will be the ones looting and pillaging. Those that live in densely populated areas will be the most vulnerable to this. To curtail this, amp up your security endeavors and preps.
For those with special needs, ensure that you have supplies and necessary medication ready for them (infants, elderly, handicapped, etc.).
I think this is the "CDC" article others were looking for---if you look closely, it is NOT the CDC putting forth these guidelines---it's the "Ready Nutrition. com" website
marsh
On TB every waking moment
Note, it looks like the author sells survival food
www.zerohedge.com
The Grim Reality About Pandemics They Don't Want You To Know: "No Country Is Prepared"
by Tyler Durden
Tue, 02/25/2020 - 19:35
Authored by Sara Tipton via ReadyNutrition.com,
It’s been 100 years since the Spanish Flu caused a global pandemic. While the WHO would like you to rest easy right now given their belief that Covid-19 is not currently a global pandemic threat, it is just a matter of time before they admit it's true. And when that day does arrive, “scientists say an outbreak of a flu-like illness could sweep across the planet in 36 hours and kill tens of millions due to our constantly-traveling population.”

According to the Daily Mail, “The report, named A World At Risk, said current efforts to prepare for outbreaks in the wake of crises such as Ebola are ‘grossly insufficient'”. It was headed by Dr. Gro Harlem Brundtland, the former Norwegian prime minister and director-general of the WHO (World Health Organization). He said in the report:
Out of the entire world, a mere 13 countries had resources and health care systems to put up a fight against a global pandemic. Among the countries ranked in the top tier were Britain, the United States, Australia, Canada, France, and Holland.
Scientists say that the size of a city and its structure can impact an influenza epidemic, meaning where you live could affect the spread of the virus. Regardless of whether flu cases rise to a wintertime peak or plateau from fall to spring, new research suggests that the size of a city itself is what influences the contours of its flu season according to Science News. Larger cities with higher levels of crowding were associated with a steady accumulation of influenza cases throughout the flu season. Smaller cities with less crowding tended to have a flu season with a more intense surge in winter, researchers report in the October 5 publication.
When a highly lethal flu pandemic comes, it will affect everyone alive today. In a related article, “Pandemic flu is apolitical and does not discriminate between rich and poor. Geographical boundaries are meaningless, and it can circle the globe within hours.” Dr. Gupta goes on to explain that when most people hear “flu”, they think of seasonal flu, but pandemic flu is “a different animal, and you should understand the difference.”
Preparations start at home
So just how do we prepare for a possible pandemic? A big concern with pandemics is that supplies would be quickly exhausted leaving many unprepared to handle the ordeal. This will only fuel a more chaotic situation. These concerns are not new to most governments and steps have been taken to ensure communities are prepared and are able to contain most epidemics.
Which such a large-scale emergency, it is difficult to know where to start and the best answer this author can give you is to start at home. We can’t control if or when governments decide to prepare, but we can control when and what we, as individuals need to protect our families.
This a suggested list of supplies to help you combat a pandemic based on the best-selling book, The Prepper’s Blueprint. The preparedness manual offers real-world advice for preppers of all levels and stages to help gear up for a pandemic.
The following is a list of pandemic supplies for your home:
In addition to having some necessary supplies on hand, you’ll also want to do the following:
* * *
This article was originally published at Ready Nutrition™ on November 12th, 2019
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
The Grim Reality About Pandemics They Don't Want You To Know: "No Country Is Prepared"
by Tyler Durden
Tue, 02/25/2020 - 19:35
Authored by Sara Tipton via ReadyNutrition.com,
It’s been 100 years since the Spanish Flu caused a global pandemic. While the WHO would like you to rest easy right now given their belief that Covid-19 is not currently a global pandemic threat, it is just a matter of time before they admit it's true. And when that day does arrive, “scientists say an outbreak of a flu-like illness could sweep across the planet in 36 hours and kill tens of millions due to our constantly-traveling population.”

According to the Daily Mail, “The report, named A World At Risk, said current efforts to prepare for outbreaks in the wake of crises such as Ebola are ‘grossly insufficient'”. It was headed by Dr. Gro Harlem Brundtland, the former Norwegian prime minister and director-general of the WHO (World Health Organization). He said in the report:
No country is fully prepared for the mayhem a pandemic flu can cause“The threat of a pandemic spreading around the globe is a real one. ‘A quick-moving pathogen has the potential to kill tens of millions of people, disrupt economies and destabilize national security.’”
Out of the entire world, a mere 13 countries had resources and health care systems to put up a fight against a global pandemic. Among the countries ranked in the top tier were Britain, the United States, Australia, Canada, France, and Holland.
Scientists say that the size of a city and its structure can impact an influenza epidemic, meaning where you live could affect the spread of the virus. Regardless of whether flu cases rise to a wintertime peak or plateau from fall to spring, new research suggests that the size of a city itself is what influences the contours of its flu season according to Science News. Larger cities with higher levels of crowding were associated with a steady accumulation of influenza cases throughout the flu season. Smaller cities with less crowding tended to have a flu season with a more intense surge in winter, researchers report in the October 5 publication.
When a highly lethal flu pandemic comes, it will affect everyone alive today. In a related article, “Pandemic flu is apolitical and does not discriminate between rich and poor. Geographical boundaries are meaningless, and it can circle the globe within hours.” Dr. Gupta goes on to explain that when most people hear “flu”, they think of seasonal flu, but pandemic flu is “a different animal, and you should understand the difference.”
Preparations start at home
So just how do we prepare for a possible pandemic? A big concern with pandemics is that supplies would be quickly exhausted leaving many unprepared to handle the ordeal. This will only fuel a more chaotic situation. These concerns are not new to most governments and steps have been taken to ensure communities are prepared and are able to contain most epidemics.
Which such a large-scale emergency, it is difficult to know where to start and the best answer this author can give you is to start at home. We can’t control if or when governments decide to prepare, but we can control when and what we, as individuals need to protect our families.
This a suggested list of supplies to help you combat a pandemic based on the best-selling book, The Prepper’s Blueprint. The preparedness manual offers real-world advice for preppers of all levels and stages to help gear up for a pandemic.
The following is a list of pandemic supplies for your home:
- One month supply of emergency foods that require no refrigeration.
- Store 1 gallon of water per person per day, in clean plastic containers. Avoid using containers that will decompose or break, such as milk cartons or glass bottles.
- Plastic sheeting
- 2-3 small wastebasket or a bucket lined with a plastic garbage bag (to dispose of clothing, soiled supplies, etc.)
- Gallon-sized zip-loc bags
- Portable toilet with disposable liners
- Supply of nonprescription drugs and pain relievers
- Cold medicines and decongestants
- Stomach remedies
- Duct tape
- Anti-diarrheal medication
- Essential oils
- Vitamins that have immune-boosting enhancers
- Fluids with electrolytes
- Bleach or disinfectant
- Soap
- Tissues
- Garbage bags to collect soiled clothing and bedding before they are washed.
- A thermometer
- Protective eye gear and/or face shield
- nitrile gloves
- Tyvek protective suit and shoe covers
- Disposable cleaning gloves (in quantity)
- Hand wipes
- Alcohol-based hand sanitizers or homemade hand sanitizer supplies
- Protective clothing
- Disposable aprons or smocks (at least 2 cases)
- Duct tape for sealing off doorways and vents
- Disposable nitrile gloves (2-3 boxes)
- Garbage bags
- N95 masks or N100 respirator masks for use when the sick person is coughing or sneezing (can be purchased at hardware stores and some drugstores)
In addition to having some necessary supplies on hand, you’ll also want to do the following:
- Store a one month supply of water and food. During a pandemic, if you cannot get to a store, or if stores are out of supplies, it will be important for you to have extra supplies on hand.
- Periodically check your regular prescription drugs to ensure a continuous supply in your home.
Have any nonprescription drugs and other health supplies on hand, including pain relievers, stomach remedies, cough, and cold medicines, fluids with electrolytes, and vitamins. - Talk with family members and loved ones about how they would be cared for if they got sick, or what will be needed to care for them in your home.
- Prepare a sick room for the home to limit family member’s exposure to the virus.
* * *
This article was originally published at Ready Nutrition™ on November 12th, 2019
Countrymouse
Country exile in the city
My son pulled the CDC telebriefing off of reddit.
https://www.reddit.com/r/China_Flu/comments/f9himd View: https://www.reddit.com/r/China_Flu/comments/f9himd/cdc_telebriefing_for_covid19/
Am listening to it now...35 mins long and 6.7 mb small file.
Just backing up what others have posted here..will still wait on "printed copy" though. Will have more effect on "others" that we know and turn their heads and smile and roll their eyes when we bring it up.
Is this the Senate hearing on Coronavirus today? Or some other teleconference?
What blew me away was her ADMITTING, at the 1:01 mark, that "new cases of covid19 are appearing without ANY KNOWN SOURCE OF EXPOSURE."
PLEASE do let me know (PM me) when your WRITTEN copy of this comes up? (I doubt I'll just "find" it in this MAMMOTH thread)
Ragnarok
On and On, South of Heaven
Can you imagine under a rationed socialist medicare for all what the numbers could look like?
Sure... China ... but only the REAL numbers...
Last edited:
marsh
On TB every waking moment
Zerohedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
NYT: "The Coronavirus Is Not A Civilization-Ender But..."
by Tyler Durden
Tue, 02/25/2020 - 17:35
Just because the New York Times Opinion Section is a perennial object of ridicule by both the right and the left doesn't mean its writers don't occasionally make a good point.
And today, we'd like to draw our readers' attention to a column published Tuesday by Ross Douthat, a member of the NYT's editorial board.
As Douthat points out, the outbreak has put Democrats, and liberals more broadly, in a difficult position. Eager to jump at every opportunity to criticize President Trump, many are secretly hoping the outbreak gets worse in the US because it could hurt Trump's chances of reelection. Many, including top Dems like Schumer, Pelosi etc., have already accused the administration of being unprepared and not doing enough.

But if the outbreak does get worse, it could deal another savage blow to the system of global frictionless exchange of people, goods, services and capital, by making countries more suspicious of allies and enemies alike.
This is why liberals are bashing Trump while arguing that pointing out China's failures is "racist."
Republicans also have an incentive to play down the outbreak, as Trump is doing: They need to keep the market buoyant and stave off a recession that could tilt the election in favor of the insurgent socialists backing Bernie Sanders.
In other words: The virus may not be a civilization-ender, as Douthat points out. But it could be the straw that breaks globalization's back.
* * *
Investors who figured this out last week are already cleaning up. But maybe there's still something to be learned here:
Read the text below:
A truism of our times is that media hysteria quickly envelops every major story, with social media virality and cable-news imperatives combining to make any domestic controversy feel like Watergate, if not Fort Sumter, and any international incident feel like the assassination of Franz Ferdinand — until the next story rolls around and last week’s crisis is forgotten.
So it’s been striking to watch media coverage of the coronavirus, which has now officially shaken free of its Chinese origins with outbreaks in Italy, South Korea and the Middle East, take a somewhat more muted tack these last few weeks. Of course there has been terrific reporting, much of it from my colleagues at this newspaper, on the surreal developments in the illness’s Wuhan epicenter.
But there has also been a strange lack of urgency in the arenas best known for their hysteria. Cable news has remained fixated on the presidential campaign, social media has been paranoid at the fringes but otherwise calm or even oblivious, our president (not typically one for threat deflation) expressed confidence that Chinese containment and spring warmth would suffice to halt the virus’s spread, and respectable opinion has circulated stern warnings about overreaction, xenophobia and panic.
The curious absence of hysteria probably reflects an interplay between polarization and ideological preconceptions. The political right would normally react to the menace of a viral outbreak in a major geopolitical rival with demands for quarantine and a zealous government response. But with a nationalist Republican president enjoying the benefits of a long economic expansion, there has been a strong partisan incentive to play down or ignore the seriousness of the virus’s threat to supply chains, the Dow, the country’s gross domestic product.
Liberals have partisan incentives that run the other way, toward emphasizing the White House’s unpreparedness in the face of a clear and present threat. But these incentives have so far been outweighed by liberalism’s ideological bias toward global openness, its anxiety about saying or doing anything that might give aid and comfort to anti-globalization forces, its fear of ever sounding too, well, Trump-y in the face of foreign threats. Thus the liberal instinct toward minimization: It’s not much worse than the flu, panicking makes things only worse, don’t spread conspiracy theories about its origins, racism toward Chinese people is the real danger here.
As of this week, with the virus finally infecting the stock market, this bipartisan minimization looks like a serious mistake. The coronavirus is not a civilization-ender, not Stephen King’s Captain Trips come for us at last, but it’s increasingly obvious that we do have a lot to fear from it, both medically and economically — and the American response seems to lag substantially behind where we should want to be right now.
The reasonable medical fears center on what is unknown as much as what is known. Because this disease broke out in a totalitarian regime, under circumstances that even China’s government now admits are more uncertain than the pious certainty offered for weeks, our knowledge of infection rates and death rates has likely been corrupted from the beginning, by misinformation and ignorance alike.
We know enough to know that most people who get it will survive it, which is good news. But we don’t know how many people get infected, how long it incubates, whether spring or summer weather will actually impede its spread. We also don’t know how many people are carriers without knowing it, and thus how easily it might move along vectors that don’t require a chain of clearly sick people running back to its point of origin. (The outbreaks outside China, in Italy especially, suggest a longer incubation period and a lot more silent contagion than had been previously hoped.)
The extreme measures that have been taken to contain the disease inside China promise all kinds of global breakdowns if they endure there and spread around the world. The supply chains that now bind our world system have never been tested in a severe pandemic, and one can extrapolate forward from China’s developing economic slowdown, and from slow-building delays and shortages worldwide, to a scenario where the coronavirus finally brings the post-2008 expansion to a grinding, deglobalizing halt.
Perhaps the worst can be averted, but these scenarios have been obvious from early in the epidemic — and so has the possibility that underreaction could make things worse, that a bias toward stability and reassurance could lead to darker outcomes in the end. It wouldn’t be the first time: As Ari Schulman wrote in The New Atlantis in 2015, during the previous year’s Ebola outbreak, the C.D.C.’s determination to reassure the public led to messaging “based on fragmentary evidence” that other evidence qualified or contradicted and left nurses caring for Ebola patients wearing only surgical masks instead of respirators; only after two nurses were infected were the guidelines changed. The World Health Organization’s response to the Ebola outbreak was delayed by fears that declaring an emergency “could anger the African countries involved, hurt their economies, or interfere with the Muslim pilgrimage to Mecca.”
From what we can tell, the coronavirus outbreak in China followed a similar pattern of “all is well” folly and insufficient first response. But in the United States, too, the “we have nothing to fear but fear itself” messaging seems inapt, given that America’s slow internal response, our apparent failure so far to expand testing beyond those who seem most obviously exposed, means that we have no way of knowing whether and how many cases are already circulating here. We may have an Italian scenario on our hands already, disguised as normal flu cases, normal flu deaths; given the still-limited scale of United States testing, there is no way to be sure, and if we escape a major outbreak, it will be more from luck than prudence.
So already, the virus has exposed a clear weak spot in what you might call the liberal-globalist imagination: an overzealous “remain calm” spirit in the face of the real risks of a hyper-connected world.
And behind that weakness lurks a structural danger for the globalist project. For the last few years there’s been a lively policy debate about the wisdom of exporting so much of the American industrial base to Asia, but it’s mostly revolved around national-security questions — what would it mean in a war with China, etc. But it turns out that you don’t need a conflict in the Taiwan straits to make the entire China-United States economic arrangement look reckless or vulnerable or unwise; you could just need one significant mutation, of one novel flu-like sickness.
But before populists crow their vindication, we need to see how our populist president handles any of this. If globalism’s weakness is technocratic naïveté, populism’s faults are ignorance, incompetence and paranoia. Nothing about President Trump’s response so far instills confidence that he’s ready for the kind of crisis that Candidate Trump would have been quick to recognize and politically exploit. And the fact that Rush Limbaugh spent yesterday declaring that the coronavirus is no worse than the common cold, and that it’s “being weaponized” by the press “to bring down Donald Trump” — well, that doesn’t instill confidence that pressure from the right will force Trump to take the outbreak seriously.
By coincidence I’m writing this column from an airport, about to embark (hand sanitizer in my pocket) on a small tour for a new book whose argument, in part, is that the Western world may be sustainably decadent — meaning that for all our gridlock, stagnation and decay, the cushion of our wealth, the weakness of our rivals and the tranquilizing effect of virtual entertainments make continued stagnation much more likely than true crisis or collapse.
I wasn’t expecting to have my thesis tested this directly while I’m literally out expounding on it. But make no mistake: The coronavirus is a test, targeted precisely to the globalized order’s points of fracture and the mix of misgovernment and mistrust associated with the populist-establishment stalemate in the West.
I believe in my own thesis enough to assume that we’ll muddle through, in the end, with (God willing) not too much damage, not too many deaths. But for better or worse we may know a lot more about the resilience of our world-system, the sustainability of our decadence, by the time the paperback comes out.
Texican
Live Free & Die Free.... God Freedom Country....
I posed a question a few days back and don't remember an answer - Does marijuana smoke have the same effect on ACE-2 receptors as tobacco smoking? What about e-cigarettes? (Doesn't tobacco increase the receptors or does it just gum them up? I thought it was increase as they were saying ex-smokers were also at risk.)
Smoking marijuana is no different to damage to the lungs as are cigarettes.... The amount of smoking from a person smoking one joint a day still happens but not as severe as the person that smokes 1 to 2 or packs of smokes a day....
Damage from smoking is cumulative.... Those that have quit smoking will start to slowly improve and the improvement is still dependent on the amount a person smoked thru the years....
The damage from e-cigs is still being determined but e-cigs are damaging to the body and lungs....
Texican....
John Deere Girl
Veteran Member
Did you check Walmart? They had huge boxes at our local store.When my husband looked, all he could find were 10 oz packages---I know the large Carnation boxes I used to get must have weighed 5 pounds at least! Doesn't anyone still make them that big?
jward
passin' thru
I'd feel more encouraged if they also had found a way to force this to present with fever! 
EndGameWW3
@EndGameWW3
1m
Navy’s 7th Fleet to screen all personnel boarding ships amid coronavirus threat
View: https://twitter.com/EndGameWW3/status/1232552164658176000?s=20
EndGameWW3
@EndGameWW3
1m
Navy’s 7th Fleet to screen all personnel boarding ships amid coronavirus threat
View: https://twitter.com/EndGameWW3/status/1232552164658176000?s=20
jward
passin' thru
Walmart also carries, at least mine does, some Anderson farm LTS products- presumably milk is part of that product line.Did you check Walmart? They had huge boxes at our local store.
Esto Perpetua
Veteran Member
Never let a crisis go to waste right? Our side could use this for the betterment of all instead of the destruction of our nation.I am comfortable right now assuming the 70% infection with a 10% mortality. Actually I feel that is pretty well padded, even. Till I see some 'man on the street' testing, I process the event as Spanish Influenza-esque event. Certainly a time in which our generation will face shared burdens and sacrifice. Also the opportunities, if we choose not to waste them, to make some needed changes. Globalism Kills! Bring our manufacturing base HOME! Borderless lands KILL! etc etc etc
jward
passin' thru
Tell ya what, if we DONT we damn well deserve what we get, and we will be no different than the mewling masses waiting for govt teat to come rescue us : (Never let a crisis go to waste right? Our side could use this for the betterment of all instead of the destruction of our nation.
Are there any theories on why this is hitting Iran so much harder than Germany, where it was contained pretty quickly? Government, hygiene, smoking, health, air pollution, genetics? Italy is hit, too, but not as bad, yet, as Iran. You know it's here, too, but nothing on the radar. Look at all the Chinese students who are here in our schools and the tourists. It's here. It's very curious or we are very blessed.
Rucus Sunday
Veteran Member
Request for AO (area of operations) update reports
When you're giving a grocery shopping/recon type of update ...
Please include WHERE YOU LIVE
It does no good to say "everything calm here" IF I DON'T WHERE "HERE" IS!
When you're giving a grocery shopping/recon type of update ...
Please include WHERE YOU LIVE
It does no good to say "everything calm here" IF I DON'T WHERE "HERE" IS!
Are there any theories on why this is hitting Iran so much harder than Germany, where it was contained pretty quickly? Government, hygiene, smoking, health, air pollution, genetics? Italy is hit, too, but not as bad, yet, as Iran. You know it's here, too, but nothing on the radar. Look at all the Chinese students who are here in our schools and the tourists. It's here. It's very curious or we are very blessed.
Iran...
Eat with right hand, wipe with left hand.
No soap.