This fella's worth a daily read, imho---
So you think you’ve about to be in a pandemic?
Posted on
February 25, 2020Author
Ian M Mackay, PhD (EIC)Leave a comment
by
Ian M Mackay, PhD and
Katherine E Arden PhD
The
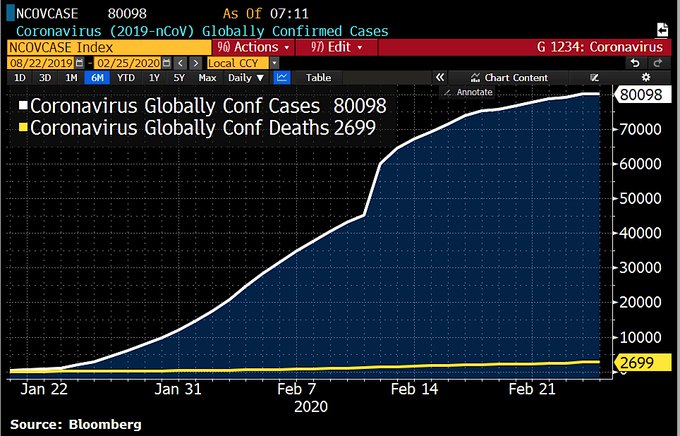
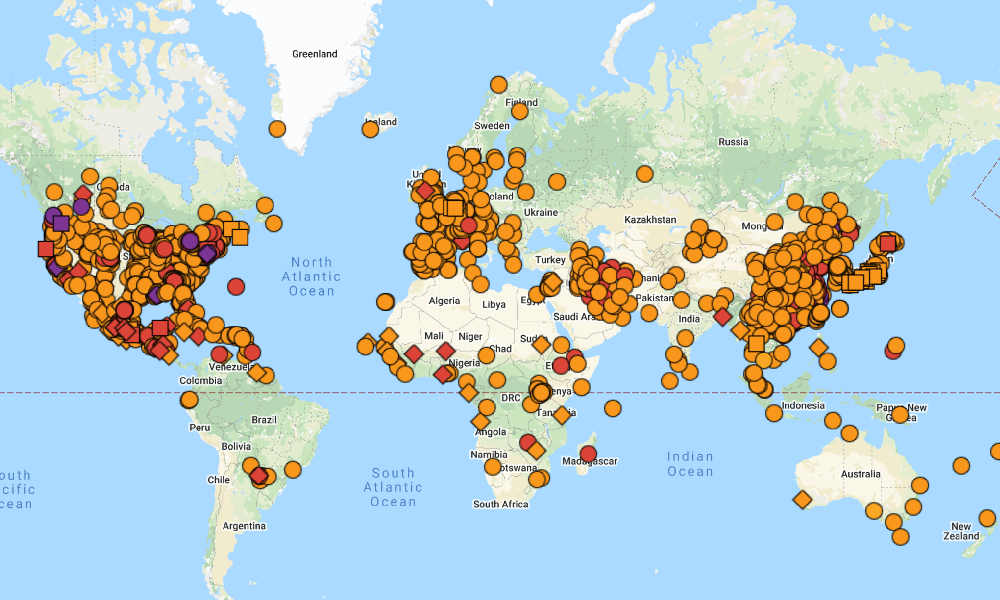
severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 [1]) has spread to over 30 countries and regions outside mainland China. Currently, disease spread in Singapore is being slowed by their expertise but new case numbers in
South Korea,
Italy and
Iran, and the wide national distribution of cases in
Japan are all signs that the virus is ahead of our efforts to contain it.
Let’s go shopping. But bit by bit – not in a rush.
Photo by
Daria Volkova on
Unsplash We’re not in a pandemic now
For now, you are more than likely
not living in an area experiencing widespread community transmission of SARS-CoV-2. If more cases of coronavirus disease 2019 (COVID-19) keep rapidly appearing, and more of them can’t be traced to existing transmission chains, the efforts in some countries to contain COVID-19 will have failed.
At some point, we’ll be in the main phase of a
pandemic; epidemics of an efficiently transmitting pathogen spreading widely within the community of two or more countries, apart from the first one to report it.[1] A pandemic doesn’t necessarily mean the disease is severe. And let’s face it if we don’t start using this possibly scary word and talking about and planning for the possibilities
now – how much more panic and fear will result because we were taken totally by surprise?
For once, let’s get ahead of what’s coming.
Assumptions and severity
This post is based on the
assumption that a pandemic will occur at some point and that Wave 1 will impact us, wherever we live, in the coming weeks and months.
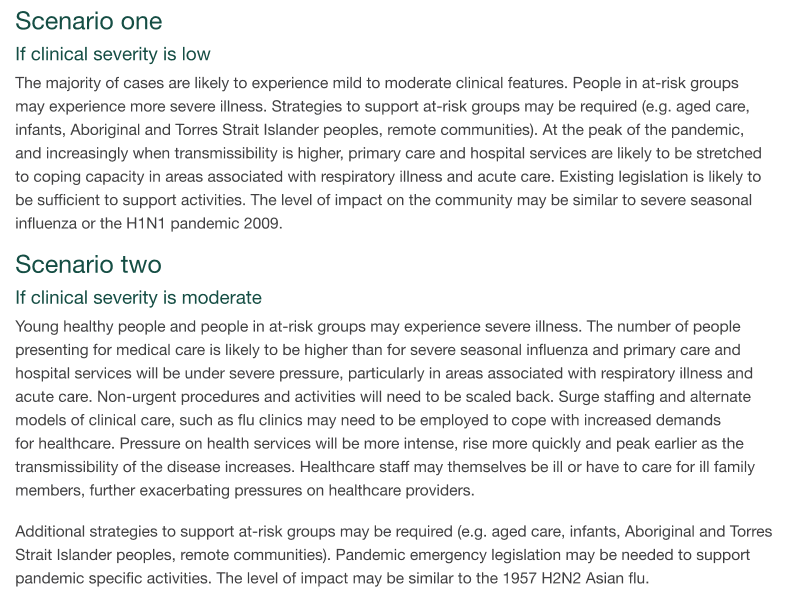
We don’t know for certain how severe a COVID-19 pandemic will be. We may be able to assume it’s a mild or perhaps moderate pandemic, not a severe one, according to definitions in the Australian Health Management Plan for Pandemic Influenza scenarios.[4] But we won’t know for sure until we see spread in countries that ask questions, define cases, and test for SARS-CoV-2 in the same way that we do.
From AHMPPI.[4]
We know that SARS-CoV-2 is effectively transmitted among humans but it may take longer for symptoms to show up in the next infected person than it does for seasonal influenza (“silent” or unnoticed shedding may happen). We also know there are no antivirals or vaccines at the time of writing and we are pretty sure that our entire population is likely to be vulnerable to infection because it doesn’t have any immunity to their new virus.
Planning now and doing something means we can control how well we cope with some of what may be coming.
If we see events cancelled or schools closed we can rest assured that this is to slow down spread, not something scarier. Hopefully, this will be clearly explained by authorities at the time.
While closures and cancellations are possible, they are by no means a sure thing. We don’t know how mild or severe SARS-CoV-2 will be, and each region will make their own – probably slightly differing – decisions about what is appropriate – and enforceable. Having a think now about how we might respond in these situations will help decisions come faster if we get to that point.
Thanks to the expert commentary of Dr Jody Lanard and Dr Peter Sandman,
in the last post, we already have some excellent ideas about what information we should be listening for, from health authorities communicating to the wider community.
What we might see happen if many get sick
If we enter into a pandemic, large numbers of people will be sick. Even if that’s just staying home with a fever and bad cough for a week. If COVID-19 is more severe, that will have a greater impact.
And when one family member is sick, one or more others may be involved in their care, removing more people from the workplace. The same effect may result if children being excluded from school. In a worst-case scenario, widespread illness may mean too few workers to drive trucks and trains, buses and taxis, run water treatment, electricity or other government services, teach at schools or staff hospitals. This didn’t happen in Australia during the 2009 H1N1 “swine flu” pandemic. But supply chains may be impacted in a number of ways.
Authorities will try to slow the speed of COVID-19 to prevent hospitals – which are essential to care for the sickest people – from being overloaded. Public gatherings – sports events and concerts – as well as schools and childcare centres, could be postponed or closed. All of which aims will be to keep people apart, making it harder for the virus to spread quickly. Again, these decisions will differ between places, and may not even have to be made.
Measures which slow the peak (1) and “flatten the curve” (2) will delay and spread out the pressure on essential healthcare function and supply chains. [3]
Once we have a vaccine, we can mitigate the impact of SARS-CoV-2, but we’re quite some way from having a safe vaccine.
Planning for everything
A lot of the planning that is going on in many places worldwide right now revolves around supporting essential services, using the numbers we have to predict the load on hospitals and to model a myriad of impacts on daily life; planning for the worst and hoping for the best.
Everyone knows the precise numbers of cases and deaths are not as precise as we’d like them to be. This is where modelling gives the authorities options – from most likely to happen, to least likely. From least concerning outcomes to the most devastating ones. And we plan accordingly. In this process, a lot of guidelines and plans and documents get written, but few of them are of use to you (or us) as members of the wider community.
It seems to take a while to get to around talking to the community about what they can do. Part of that’s because of how consumed with work many are right now because this epidemic is still only 8 weeks old; an infant, yet one that moves like a teenager who just discovered caffeine. And yet, late last week and over the weekend, the signal fires of pandemic awareness and increased communication started to light.
But what can we plan for and do?
Let’s break this into two main categories.
- Reducing our risk of being infected
- Reducing the chance we will run out of essential foods and goods
Reducing our risk of being infected
We can do a few things and we’ve probably heard them all before. They won’t guarantee to protect us from infection, but they can reduce our
risk of infection. These are just as useful for avoiding influenza (flu) virus infection during flu season and for dodging SARS-CoV-2, once your local community is known to have it circulating.
REMEMBER: As long as the virus circulates, and as long as you have never been infected, you are susceptible to infection resulting in COVID-19. This will be the case for the rest of your life until you have been infected which should protect you from severe disease. COVID-19 is mostly a mild illness but can cause severe pneumonia in approximately 20% of cases, leading to hospitalization for weeks and in a portion of these cases, to death.
World Health Organization.[3]
These are things we can do to reduce our risk of SARS-CoV-2 infection.
- Stay at least 2m away from obviously sick people.
We’re trying to avoid receiving a cough/sneeze in the face, shaking hands, or being in the range of droplet splatter and the “drop zone”
- Wash your hands for 20 seconds & more frequently than you do now
Soap and water and then dry, or an alcohol-based hand rub, and air dry
- Try not to touch your face.
There is a chance your unwashed fingers will have a virus on them and if you touch/rub your mouth, nose or eyes, you may introduce the virus and accidentally infect yourself. Practice this; get others to call you out when you forget. Make it a game.
While a mask
seems like a good idea, and when used by professionals it does protect from infection, it can actually give inexperienced users a false sense of security. There isn’t a lot of good evidence (still!) that shows a mask to reliably prevent infection when worn by the public at large. They
are useful to put on a sick person to reduce their spreading of the virus.
If you or a loved one becomes sick, follow the practices of the day. Call ahead before going to a Doctor, fever clinic or hospital and get advice on what to do. Hopefully, this message is already out there and we’ll see it more once transmission of the virus is widespread.
Reducing our risk of running short of food and important goods – the 2-week list
What we’re looking at here is trying to minimize the impact of any shortages of goods we rely on having at the grocery store or at the end of an online ordering system.
Dried fruit. It lasts and is nutritious.
Photo by
VisionPic .net from
Pexels
But don’t panic buy and don’t hoard!
Most of the world is not seeing any widespread ongoing transmission of SARS-CoV-2, so now is a great time to make list, label up a “Pandemic Stash” box, and begin to slowly fill it with items that won’t go off and that you won’t touch unless needed. Buy a few of the things each weekly shop. Don’t buy things you won’t eat later, don’t hoard and don’t buy more than you’ll need for a 2 week period. We’re not talking zombie apocalypse and we very probably won’t see power or water interruptions either.
Our household is trying to get food that fulfil a need for carbohydrate, protein, and fibre. We also want supplies for caring for the sick (or for when sick yourself) and cleaning supplies to try to reduce the spread.
Below we list things we’ll need to have in case of a more major interruption to supply; a stock that will last 2 weeks. Some of these things will last much longer and include items that may not be a top priority for authorities to keep stocked:
- Extra prescription medications, asthma relief inhalers
Some of these may be a problem, so talk to your doctor soon.
- Over-the-counter anti-fever and pain medications
paracetamol and ibuprofen can go a long way to making us feel less sick
- Feminine hygiene products
- Family pack of toilet paper
- Vitamins
In case food shortages limit the variety in your diet
- Alcohol-containing hand rub
- Soap
- Household cleaning agents
Bleach, floor cleaner, toilet cleaner, surface cleaning spray, laundry detergent
- Tissues, paper towel
- Cereals, grains, pasta
- Tinned food – fish, vegetables, fruit
- Oil, spices and flavours
- Dried fruit and nuts
- Ultra-heat treated or powdered milk
Ian is not drinking black coffee, no matter what
- Soft drink or candy/chocolate for treats
- Think about elderly relative’s needs
Their medications, pets, pandemic stash, plans for care (see later)
- Pet food and care
Dry and tinned food, litter tray liners, medicines, anti-flea drops
The last-minute fresh list
In a more severe pandemic, supply chain issues may mean fresh food becomes harder to get. So this list is an add-on to the one above, and its items should be the
last things to buy if you have a hint of when supplies might slow or stop for a (hopefully short) time.
- Bread, wraps
- Meat for freezing
- Milk
- Eggs
- Yogurt
- Vegetables, fruit
The elderly and COVID-19
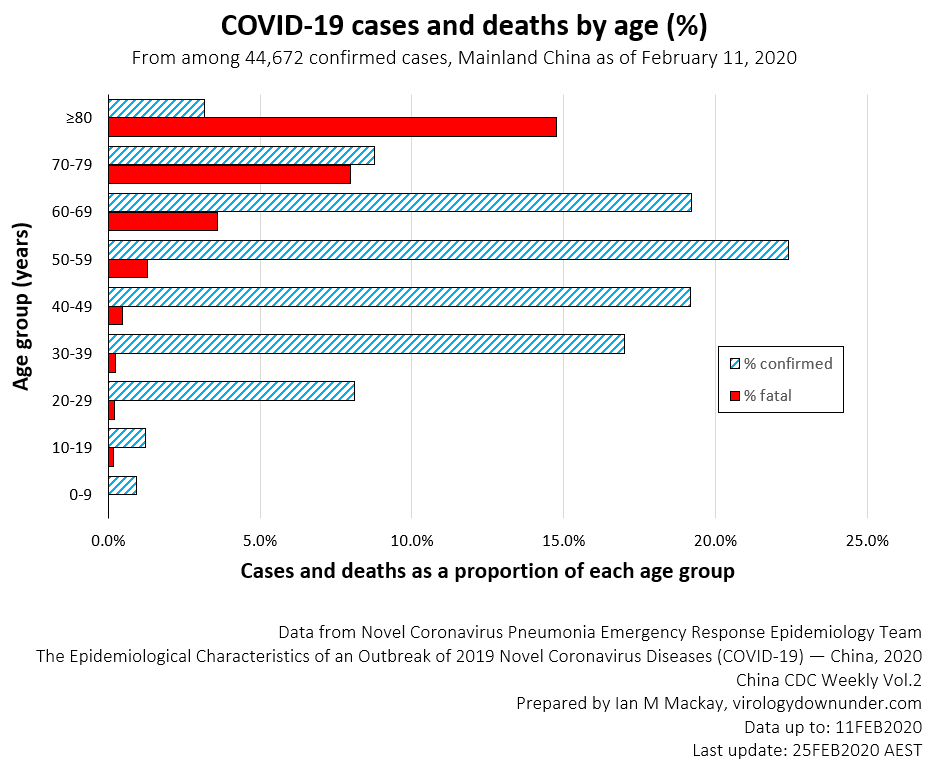
To date, looking at data from China (below), most (94%) deaths from COVID-19 have occurred in those aged over 50 years of age, with more than half (51%) in those aged over 70 years. The age group most at risk for death are those aged over 80 years.
Older people with comorbidities have experienced higher proportions of death than those with no comorbidities. Most cases identified in mainland China – 80.9% of them – even with the more severe case catching that China has favoured – have been classified as mild. This is good news although 20% is still a lot of “severe” disease. Mild cases recover in about 2 weeks from the time they showed symptoms, while severe cases can take 3 to 6 weeks to recover.
Infographic of the largest study of cases from China.[1]
Because of this, we may see a big impact on our elderly population, both in terms of hospitalisation and death. Residential aged care is likely to suffer and visits to loved ones may be restricted to keep them safe. If you have loved ones in an aged care facility, ask the facility about its plans for keeping their residents safe from flu (a similar situation) and whether they have thought about what they will do if SARS-CoV-2 is spreading widely.
It will be important to check that your parents and grandparents have prepared a
Will and have considered an
Enduring Power of Attorney in case they are unable to make care-based decisions for themselves. These aren’t fun to organise or think about, but they’re important whether we see a COVID-19 pandemic or not, so just use this as a reminder to get it done.
Pandemic is a word, how we react to it is down to us
We all want to have some control over our lives but when a virus comes knocking as this one is, we feel the loss of that control. The lists above are something we can
actually do.
We’re working on this in our household now, bit by bit. The lists have helped us all focus on how that “thing going on in that faraway country” will impact us when it comes to our neighborhood. This process has already made things a little more familiar and a little less unknown and scary. We’ve done some things that will help. We know there are still risks but we’ve talked about them, calmly, as a family.
Of course, this doesn’t
remove the many unknowns, but we’re sure we’ll gradually reduce those as science gets us more answers. Hopefully, these answers will bring good news; lower death rates, effective antiviral drugs, and new vaccines.
We do have some experience of a pandemic and it wasn’t panic-worthy. The pandemic of H1N1 “swine flu” in 2009 had some unhappy consequences, but it was by no means a zombie apocalypse.
China has bought us time to prepare. Let’s not waste any more of it. Instead, let’s get our planning hats on and all work the problem together. This is one of those rare times when we’re unarguably all in this together.
SARS-CoV-2 doesn’t care about our beliefs, our sex or gender, our colour or our clothes – it just wants to make a home in our human cells.
It’s perfectly okay to be anxious about this.
But work the problem.
References
- Not so novel: numbers: around COVID-19 and SARS-CoV-2
- Advice for public
- Interim pre-pandemic planning guidance: community strategy for pandemic influenza mitigation in the United States: early, targeted, layered use of nonpharmaceutical interventions. Published Date: February 2007
https://stacks.cdc.gov/view/cdc/11425
- Australian Health Management Plan for Pandemic Influenza (AHMPPI)
August 2019
https://www1.health.gov.au/internet/main/publishing.nsf/Content/ohp-ahmppi.htm
Hits: 0
Categories
Communication,
Coronavirus,
Pandemic
by Ian M Mackay, PhD and Katherine E Arden PhD The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 [1]) has spread to over 30 countries and regions outside mainland China. Currently, disease spread in Singapore

virologydownunder.com